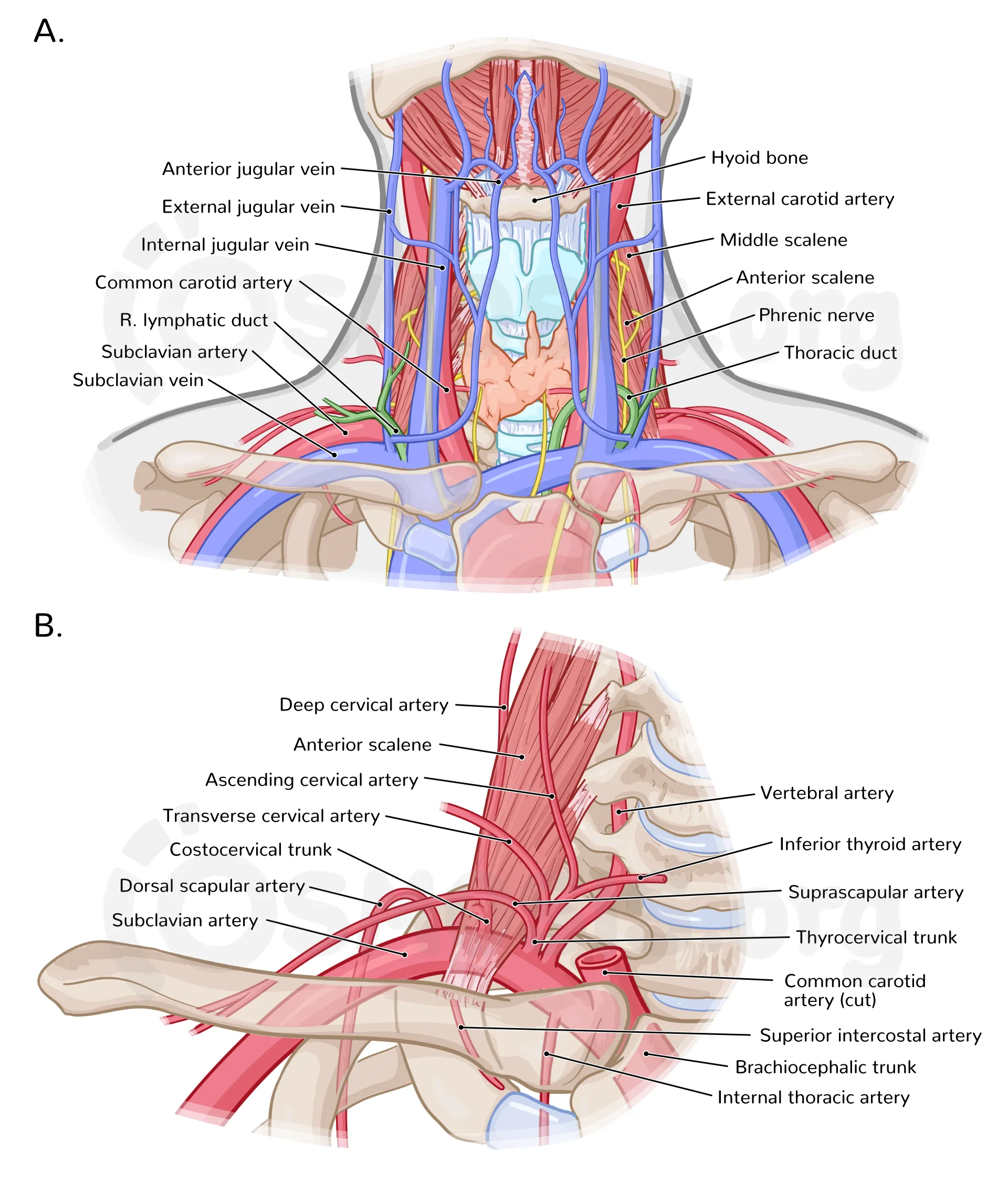
Neurovascular Structures of the Neck Anatomy Clinical Importance and Exam Guide
Explore Related Content
- Home Latest medical posts
- Sitelinks Index Complete site map
- Upload Medical Content Share clinical pearls
- More ANATOMY Posts Browse related content
- Reviews & Suggestions Community feedback
- Help & FAQ Upload & SEO tips
- More from this Author View all posts
- About Streamora Medical learning hub
Related Posts
Posts with similar category or tags for stronger sitelinks & internal backlinks.
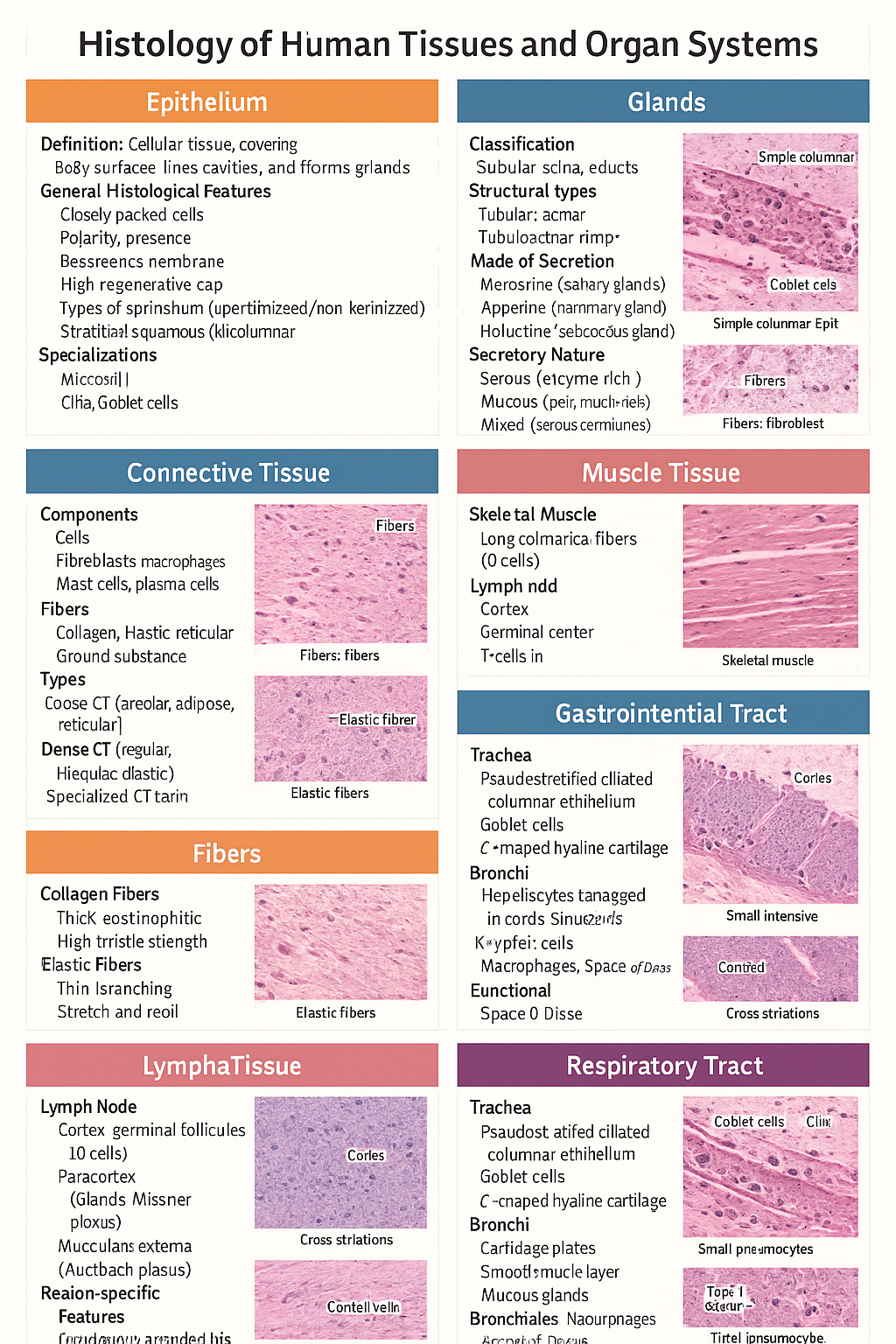
Histology of Epithelium, Connective Tissue, Muscle, Cartilage, Glands, GIT, Liver and Respiratory Tract
Below is a **single-place, SEO-optimized, exam-ready histology guide** covering **epithelium, glands, connective tissue, fibers, cartilage, muscle, lymphatic system, GIT, liver, and respiratory tract**. Structured with **clear H1–H3 headings**, **high-yield features**, and **clinical correlations** for medical students and competitive exams. --- # Histology of Human Tissues and Organ Systems – Complete Guide ## Histology of Epithelium ### Definition Epithelium is a **cellular tissue** that covers body surfaces, lines cavities, and forms glands. ### General Histological Features * Closely packed cells with **minimal extracellular matrix** * **Polarity**: apical, lateral, basal surfaces * **Basement membrane** present * **Avascular**, richly innervated * High **regenerative capacity** ### Types of Epithelium * **Simple squamous**: alveoli, capillaries * **Simple cuboidal**: kidney tubules, glands * **Simple columnar**: stomach, intestine * **Stratified squamous (keratinized/non-keratinized)**: skin / oral cavity * **Pseudostratified ciliated columnar**: trachea * **Transitional epithelium**: urinary bladder ### Specializations * **Microvilli** – absorption * **Cilia** – movement * **Goblet cells** – mucus secretion --- ## Histology of Glands ### Classification * **Exocrine glands** – ducts present * **Endocrine glands** – ductless, secrete into blood ### Structural Types * **Tubular**, **acinar**, **tubuloacinar** * **Simple** or **compound** ### Mode of Secretion * **Merocrine** (salivary glands) * **Apocrine** (mammary gland) * **Holocrine** (sebaceous gland) ### Secretory Nature * **Serous** – enzyme-rich, dark staining * **Mucous** – pale, mucin-rich * **Mixed** – serous demilunes --- ## Histology of Connective Tissue ### Components * **Cells**: fibroblasts, macrophages, mast cells, plasma cells * **Fibers**: collagen, elastic, reticular * **Ground substance**: proteoglycans, GAGs ### Types * **Loose CT**: areolar, adipose, reticular * **Dense CT**: regular, irregular, elastic * **Specialized CT**: cartilage, bone, blood --- ## Histology of Fibers ### Collagen Fibers * Thick, eosinophilic * High tensile strength * Seen in tendons, ligaments ### Elastic Fibers * Thin, branching * Stretch and recoil * Found in lungs, elastic arteries ### Reticular Fibers * Type III collagen * Supportive network * Seen in lymphoid organs --- ## Histology of Cartilage ### General Features * Avascular * Chondrocytes in **lacunae** * Perichondrium present (except articular cartilage) ### Types * **Hyaline cartilage**: trachea, articular surfaces * **Elastic cartilage**: pinna, epiglottis * **Fibrocartilage**: intervertebral discs, pubic symphysis --- ## Histology of Muscle Tissue ### Skeletal Muscle * Long cylindrical fibers * **Multinucleated**, peripheral nuclei * Cross striations present * Voluntary ### Cardiac Muscle * Branching fibers * Single central nucleus * **Intercalated discs** * Involuntary ### Smooth Muscle * Spindle-shaped cells * No striations * Involuntary * Found in viscera, vessels --- ## Histology of Lymphatic System ### Lymph Node * Capsule with trabeculae * **Cortex**: lymphoid follicles (B cells) * **Paracortex**: T cells * **Medulla**: medullary cords and sinuses ### Spleen * **White pulp**: lymphocytes around central artery * **Red pulp**: sinusoids and splenic cords ### Thymus * Cortex and medulla * **Hassall’s corpuscles** * T-cell maturation --- ## Histology of Gastrointestinal Tract (GIT) ### Common Layers 1. **Mucosa** – epithelium, lamina propria, muscularis mucosa 2. **Submucosa** – glands, Meissner plexus 3. **Muscularis externa** – Auerbach plexus 4. **Serosa/adventitia** ### Region-Specific Features * **Esophagus**: stratified squamous epithelium * **Stomach**: simple columnar epithelium, gastric glands * **Small intestine**: villi, plicae circulares, Peyer’s patches (ileum) * **Colon**: no villi, abundant goblet cells --- ## Histology of Liver ### Structural Unit * **Classical hepatic lobule** * Central vein * Portal triad: hepatic artery, portal vein, bile duct ### Cellular Features * Hepatocytes arranged in cords * **Sinusoids** lined by fenestrated endothelium * **Kupffer cells** – macrophages * **Space of Disse** ### Functional Significance * Metabolism * Detoxification * Bile production --- ## Histology of Respiratory Tract ### Trachea * Pseudostratified ciliated columnar epithelium * Goblet cells * C-shaped hyaline cartilage ### Bronchi * Cartilage plates * Smooth muscle layer * Mucous glands ### Bronchioles * No cartilage or glands * Simple ciliated columnar → cuboidal epithelium ### Alveoli * **Type I pneumocytes** – gas exchange * **Type II pneumocytes** – surfactant * Alveolar macrophages --- ## High-Yield Exam Pearls * Transitional epithelium is **unique to urinary tract** * Fibrocartilage **lacks perichondrium** * Peyer’s patches are characteristic of **ileum** * Kupffer cells are **liver macrophages** * Type II pneumocytes produce **surfactant** --- If you want, I can next: * ✅ Convert this into **HTML-CSS-JS single-file notes** * ✅ Add **labeled histology images** * ✅ Generate **25 image-based MCQs** * ✅ Create **printable PDF or exam charts** Just tell me 👍
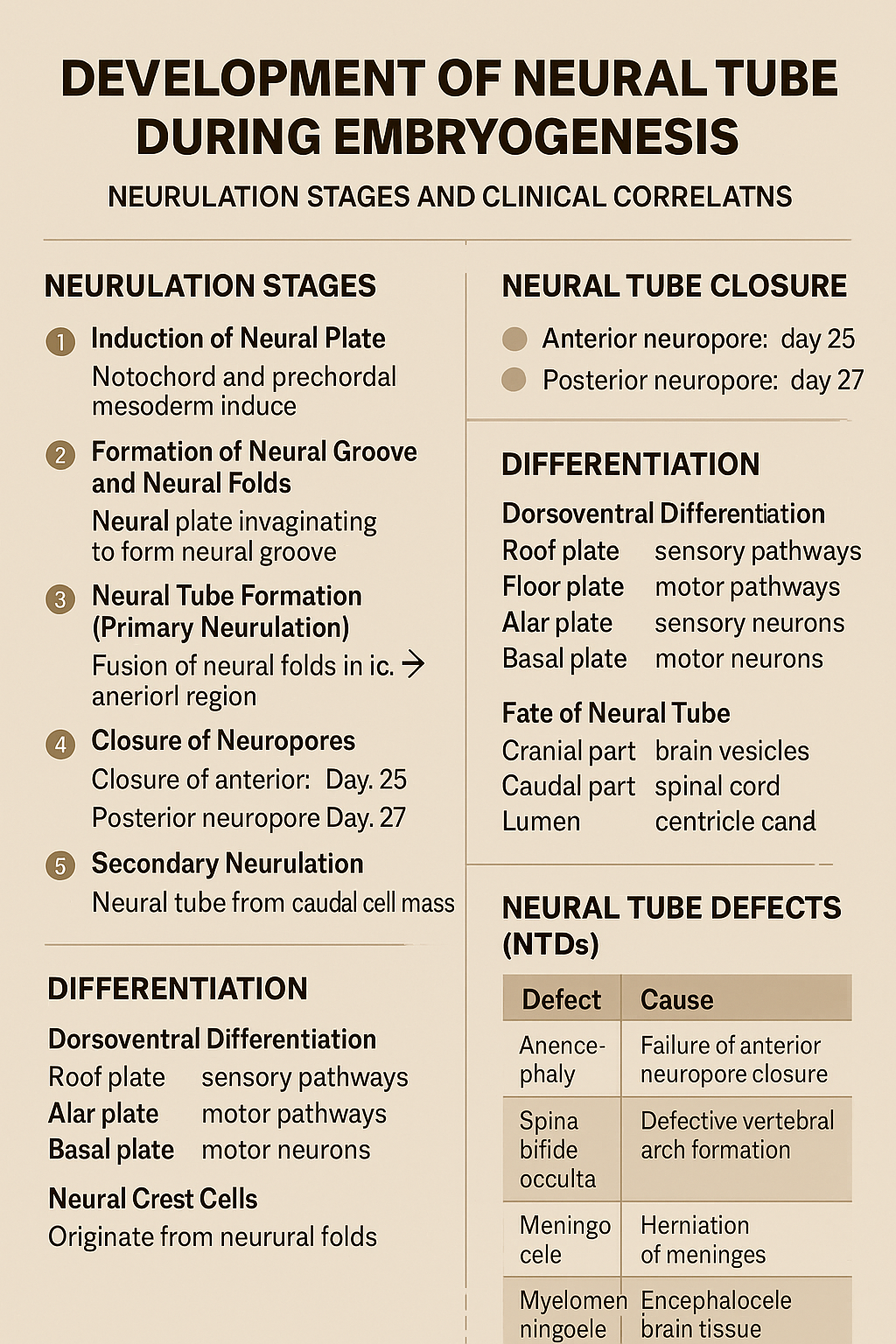
Development of Neural Tube During Embryogenesis Neurulation Stages and Clinical Correlation
## Development of the Neural Tube (Neurulation) ### **Definition** The **neural tube** is the embryonic precursor of the **central nervous system (CNS)**, forming the **brain and spinal cord**. Its development occurs by **neurulation** during the **3rd and 4th weeks of intrauterine life**. --- ## **Timeline** * **Day 18**: Neural plate appears * **Day 20–21**: Neural folds form * **Day 22**: Fusion begins in cervical region * **Day 25**: Closure of anterior (cranial) neuropore * **Day 27**: Closure of posterior (caudal) neuropore --- ## **Phases of Neural Tube Development** ### **1. Induction of Neural Plate** * The **notochord** and **prechordal mesoderm** induce overlying **ectoderm**. * Ectoderm thickens to form the **neural plate**. **Key signaling molecules**: * Sonic hedgehog (Shh) * Noggin * Chordin * Follistatin --- ### **2. Formation of Neural Groove and Neural Folds** * Central neural plate invaginates → **neural groove**. * Lateral edges elevate → **neural folds**. * Neural folds approach each other dorsally. --- ### **3. Neural Tube Formation (Primary Neurulation)** * Neural folds fuse in the **midline**, starting in the **cervical region**. * Fusion proceeds cranially and caudally. * Temporary openings remain: * **Anterior (cranial) neuropore** * **Posterior (caudal) neuropore** --- ### **4. Closure of Neuropores** * **Anterior neuropore closes (Day 25)** → brain development * **Posterior neuropore closes (Day 27)** → spinal cord development Failure of closure leads to **neural tube defects**. --- ### **5. Secondary Neurulation** * Occurs in the **caudal region (below S2)**. * Neural tube forms from **caudal cell mass**. * Important for formation of: * Conus medullaris * Filum terminale --- ## **Differentiation of the Neural Tube** ### **Neural Tube Wall Layers** 1. **Ventricular (ependymal) layer** – neuroepithelial cells 2. **Mantle layer** – gray matter 3. **Marginal layer** – white matter --- ### **Dorsoventral Differentiation** * **Roof plate** → sensory pathways * **Floor plate** → motor pathways * **Alar plate** → sensory neurons * **Basal plate** → motor neurons * **Sulcus limitans** separates alar and basal plates --- ## **Fate of Neural Tube** * **Cranial part** → brain vesicles * Prosencephalon * Mesencephalon * Rhombencephalon * **Caudal part** → spinal cord * **Lumen** → ventricles and central canal --- ## **Neural Crest Cells (Related Event)** * Originate from neural folds * Migrate extensively * Form: * Peripheral nervous system * Melanocytes * Adrenal medulla * Craniofacial cartilage --- ## **Clinical Correlation: Neural Tube Defects (NTDs)** | Defect | Cause | | -------------------- | ------------------------------------- | | Anencephaly | Failure of anterior neuropore closure | | Spina bifida occulta | Defective vertebral arch formation | | Meningocele | Herniation of meninges | | Myelomeningocele | Herniation of spinal cord + meninges | | Encephalocele | Herniation of brain tissue | **Risk factors**: * Folic acid deficiency * Maternal diabetes * Valproate exposure **Prevention**: * Folic acid 400–800 µg/day (preconception) --- ### **One-Line Exam Summary** > The neural tube forms from ectoderm by neurulation during weeks 3–4 and develops into the brain and spinal cord. If you want, I can also provide **exam-oriented MCQs, flowcharts, or comparison tables** for neurulation.
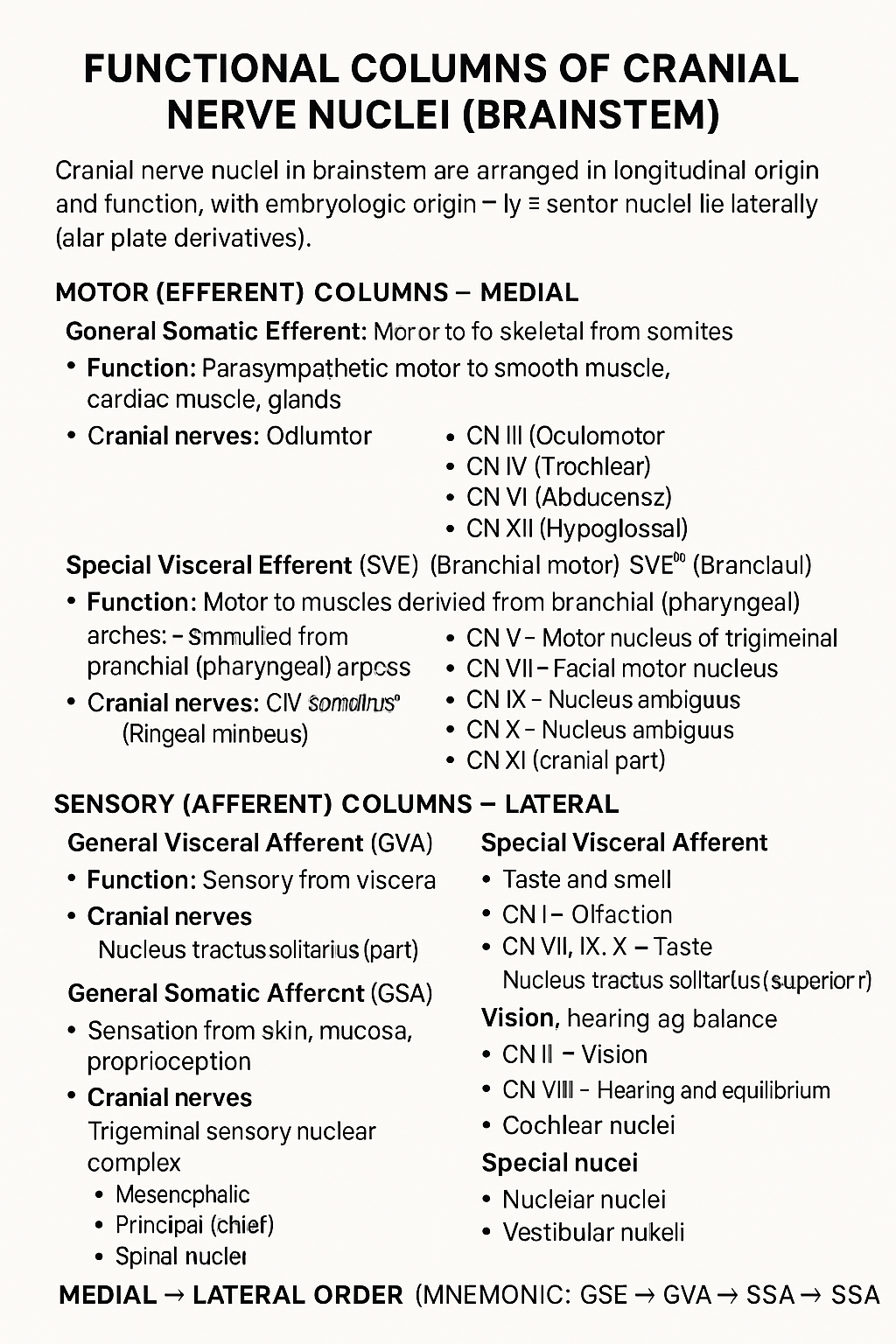
Functional Columns of Cranial Nerve Nuclei in Brainstem
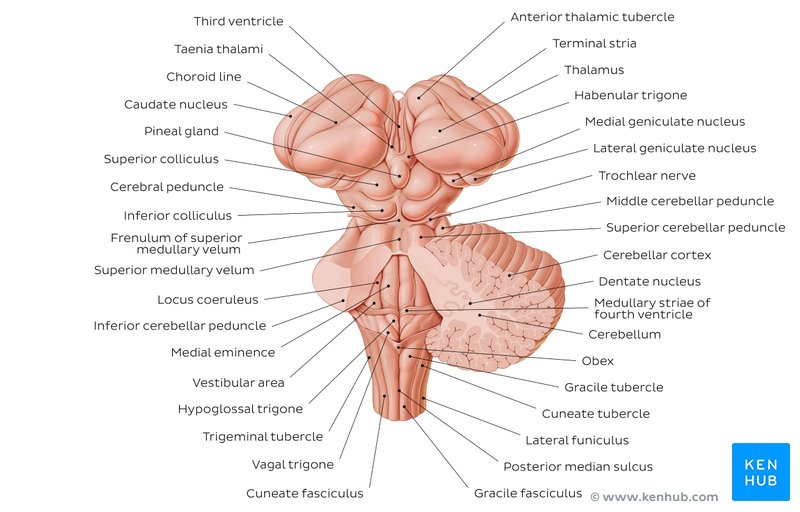
## Functional Columns of Cranial Nerve Nuclei (Brainstem) Cranial nerve nuclei in the brainstem are arranged in **longitudinal functional columns** based on **embryologic origin** and **function**. **Motor nuclei lie medially** (basal plate derivatives) and **sensory nuclei lie laterally** (alar plate derivatives). --- ## MOTOR (EFFERENT) COLUMNS – Medial ### 1. **General Somatic Efferent (GSE)** * **Function:** Motor to skeletal muscles derived from **somites** * **Muscles supplied:** Extraocular muscles, tongue muscles * **Cranial nerves:** * CN III (Oculomotor) * CN IV (Trochlear) * CN VI (Abducens) * CN XII (Hypoglossal) --- ### 2. **General Visceral Efferent (GVE)** * **Function:** **Parasympathetic** motor to smooth muscle, cardiac muscle, glands * **Cranial nerves & nuclei:** * CN III – Edinger–Westphal nucleus * CN VII – Superior salivatory nucleus * CN IX – Inferior salivatory nucleus * CN X – Dorsal motor nucleus of vagus --- ### 3. **Special Visceral Efferent (SVE)** *(Branchial motor)* * **Function:** Motor to muscles derived from **branchial (pharyngeal) arches** * **Muscles supplied:** Muscles of mastication, facial expression, pharynx, larynx * **Cranial nerves:** * CN V – Motor nucleus of trigeminal * CN VII – Facial motor nucleus * CN IX – Nucleus ambiguus * CN X – Nucleus ambiguus * CN XI (cranial part) --- ## SENSORY (AFFERENT) COLUMNS – Lateral ### 4. **General Visceral Afferent (GVA)** * **Function:** Sensory from viscera * **Cranial nerves:** * CN IX * CN X * **Nucleus:** Nucleus tractus solitarius (inferior part) --- ### 5. **Special Visceral Afferent (SVA)** * **Function:** Taste and smell * **Cranial nerves:** * CN I – Olfaction * CN VII, IX, X – Taste * **Nucleus:** Nucleus tractus solitarius (superior part) --- ### 6. **General Somatic Afferent (GSA)** * **Function:** Sensation from skin, mucosa, proprioception * **Cranial nerves:** * CN V (main) * CN VII, IX, X (small contributions) * **Nuclei:** * Trigeminal sensory nuclear complex * Mesencephalic * Principal (chief) * Spinal nucleus --- ### 7. **Special Somatic Afferent (SSA)** * **Function:** Vision, hearing, balance * **Cranial nerves:** * CN II – Vision * CN VIII – Hearing and equilibrium * **Nuclei:** * Cochlear nuclei * Vestibular nuclei --- ## MEDIAL → LATERAL ORDER (Mnemonic) **GSE → GVE → SVE → GVA → SVA → GSA → SSA** --- If you want, I can also provide: * **One-table summary (exam revision)** * **Clinical correlations** * **Simple mnemonics for each column** * **Neat labelled text diagram (ASCII-style)**
Cerebrospinal Fluid and Ventricular System Anatomy
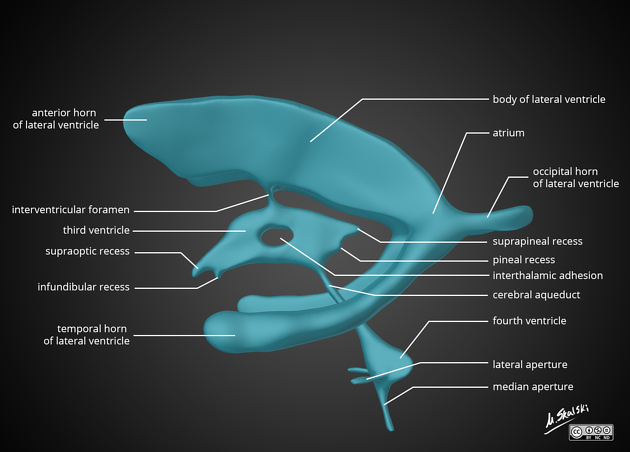
## Cerebrospinal Fluid and Ventricular System Anatomy – Complete SEO-Friendly Guide ### SEO Title **Cerebrospinal Fluid and Ventricular System Anatomy** ### Meta Description Detailed anatomy of cerebrospinal fluid and the ventricular system covering formation, circulation, absorption, functions, ventricular components, and important clinical correlations. ### Keywords cerebrospinal fluid anatomy, ventricular system brain, lateral ventricles anatomy, third ventricle anatomy, fourth ventricle anatomy, CSF circulation, choroid plexus, arachnoid villi, hydrocephalus anatomy --- ## 1. Cerebrospinal Fluid (CSF) ### Definition Cerebrospinal fluid is a **clear, colorless fluid** that circulates within the **ventricular system of the brain and subarachnoid space** surrounding the brain and spinal cord, providing protection, nutrition, and waste removal. ### Normal Volume and Pressure * Total volume (adult): **≈150 mL** * Daily production: **≈500 mL** * Normal opening pressure (lumbar puncture): **70–180 mm H₂O** --- ## 2. Formation of CSF ### Choroid Plexus CSF is primarily produced by the **choroid plexus**, a vascular structure lined by **ependymal cells**. **Locations of choroid plexus** * Lateral ventricles (body and temporal horn) * Third ventricle * Fourth ventricle **Mechanism** * Active secretion via **Na⁺/K⁺ ATPase** * Water follows osmotically * Independent of intracranial pressure --- ## 3. Ventricular System of the Brain The ventricular system consists of **four interconnected cavities** lined by ependyma and filled with CSF. --- ### 3.1 Lateral Ventricles (First and Second Ventricles) **Location** * One in each cerebral hemisphere **Parts** 1. **Anterior (frontal) horn** * In frontal lobe * Roof: Corpus callosum * Floor: Head of caudate nucleus 2. **Body** * Extends through parietal lobe 3. **Posterior (occipital) horn** * In occipital lobe 4. **Inferior (temporal) horn** * In temporal lobe * Floor: Hippocampus * Roof: Tail of caudate nucleus **Communication** * Each lateral ventricle communicates with the third ventricle via the **interventricular foramen (foramen of Monro)** --- ### 3.2 Third Ventricle **Location** * Midline cavity between the two thalami **Boundaries** * Lateral walls: Thalamus and hypothalamus * Floor: Hypothalamus * Roof: Tela choroidea * Anterior wall: Lamina terminalis * Posterior wall: Pineal region **Connections** * Receives CSF from lateral ventricles * Drains into the fourth ventricle via the **cerebral aqueduct (aqueduct of Sylvius)** --- ### 3.3 Fourth Ventricle **Location** * Between pons and medulla anteriorly * Cerebellum posteriorly **Boundaries** * Floor: Rhomboid fossa * Roof: Superior and inferior medullary vela **Openings** * **One median aperture (foramen of Magendie)** * **Two lateral apertures (foramina of Luschka)** These openings allow CSF to enter the **subarachnoid space**. --- ## 4. Circulation of CSF **Flow pathway** 1. Lateral ventricles 2. Foramen of Monro 3. Third ventricle 4. Cerebral aqueduct 5. Fourth ventricle 6. Foramen of Magendie and Luschka 7. Subarachnoid space 8. Arachnoid villi and granulations 9. Superior sagittal sinus --- ## 5. Absorption of CSF ### Arachnoid Villi and Granulations * Protrusions of arachnoid mater into venous sinuses * Act as **one-way valves** * Absorption occurs when CSF pressure exceeds venous pressure Minor absorption also occurs via: * Spinal nerve sheaths * Choroid plexus --- ## 6. Composition of CSF * Clear and acellular * Low protein * Low potassium and calcium * Higher chloride compared to plasma * Glucose ≈ 60% of plasma glucose --- ## 7. Functions of CSF * **Mechanical protection** (shock absorber) * **Buoyancy** (reduces effective brain weight) * **Nutrient delivery** * **Removal of metabolic waste** * **Maintenance of intracranial pressure** --- ## 8. Blood–CSF Barrier Formed by: * Tight junctions between **choroid plexus epithelial cells** Functions: * Regulates composition of CSF * Protects CNS from toxins --- ## 9. Clinical Correlations ### Hydrocephalus * Abnormal accumulation of CSF **Types** * **Non-communicating (obstructive):** Block within ventricular system (e.g., aqueductal stenosis) * **Communicating:** Impaired absorption at arachnoid villi * **Normal pressure hydrocephalus:** Triad of gait disturbance, dementia, urinary incontinence --- ### Raised Intracranial Pressure * Headache * Vomiting * Papilledema * Altered consciousness --- ### Lumbar Puncture * Performed at **L3–L4 or L4–L5** * Measures CSF pressure and composition --- ## 10. High-Yield Exam Points * CSF production: **Choroid plexus** * Narrowest part of ventricular system: **Cerebral aqueduct** * Largest ventricles: **Lateral ventricles** * Main absorption site: **Arachnoid granulations** * CSF volume remains constant despite high daily production --- If you want, I can also provide **MCQs (exam-oriented)**, **clinical case-based questions**, or **schema-style revision tables** for CSF and ventricles.
Brainstem Syndromes Explained With 30 High-Yield Case Scenarios and Management
## **Brainstem Syndromes Case Scenarios With Clinical Explanation and Management Guide** ### **SEO Title** **Brainstem Syndromes Explained With 30 High-Yield Case Scenarios and Management** ### **SEO Description** Comprehensive SEO-friendly guide on brainstem syndromes with 30 detailed clinical case scenarios, anatomical explanations, lesion localization, and stepwise management for medical exams and clinical practice. ### **SEO Keywords** brainstem syndromes, midbrain syndromes, pontine syndromes, medullary syndromes, weber syndrome, benedict syndrome, lateral medullary syndrome, brainstem lesion cases, neurology case scenarios, brainstem stroke management --- ## **MIDBRAIN SYNDROMES** --- ### **1. Weber Syndrome** **Case Scenario:** A 55-year-old man presents with sudden right-sided weakness and drooping of the left eyelid. Examination shows left eye ptosis, dilated pupil, and right hemiplegia. **Explanation:** Lesion in **ventromedial midbrain** affecting: * Oculomotor nerve (III) * Corticospinal tract Usually due to **posterior cerebral artery infarct** **Management:** * Acute ischemic stroke protocol * Antiplatelet therapy * Blood pressure and glucose control * Physiotherapy for hemiplegia --- ### **2. Benedikt Syndrome** **Case Scenario:** A patient has ipsilateral oculomotor palsy with contralateral tremor and ataxia. **Explanation:** Lesion in **tegmentum of midbrain** involving: * Oculomotor nerve * Red nucleus * Medial lemniscus **Management:** * Treat stroke or tumor cause * Antiplatelets or anticoagulation * Rehabilitation for ataxia --- ### **3. Claude Syndrome** **Case Scenario:** A patient presents with ipsilateral third nerve palsy and contralateral limb ataxia. **Explanation:** Combination of **Weber + Benedikt** * Oculomotor nerve * Red nucleus * Corticospinal tract **Management:** * Stroke management * Neurorehabilitation --- ### **4. Parinaud Syndrome** **Case Scenario:** Young adult with inability to look upward and light-near dissociation. **Explanation:** Lesion in **dorsal midbrain (pineal region)** Often due to pineal tumor or hydrocephalus. **Management:** * Treat raised intracranial pressure * Neurosurgical tumor management --- ### **5. Nothnagel Syndrome** **Case Scenario:** Patient has ipsilateral third nerve palsy and cerebellar ataxia. **Explanation:** Lesion of **superior cerebellar peduncle + oculomotor nerve** **Management:** * Tumor or demyelination treatment * Supportive therapy --- ## **PONTINE SYNDROMES** --- ### **6. Millard-Gubler Syndrome** **Case Scenario:** A patient shows facial paralysis on left side with right-sided hemiplegia. **Explanation:** Lesion in **ventral pons** * Facial nerve (VII) * Corticospinal tract **Management:** * Stroke care * Facial physiotherapy --- ### **7. Foville Syndrome** **Case Scenario:** Inability to abduct eye, facial weakness, and contralateral hemiplegia. **Explanation:** Lesion in **pontine tegmentum** * Abducens nucleus * Facial nerve * Corticospinal tract **Management:** * Antiplatelets * Eye care for diplopia --- ### **8. Raymond Syndrome** **Case Scenario:** Ipsilateral lateral rectus palsy with contralateral hemiplegia. **Explanation:** Lesion affects: * Abducens nerve * Corticospinal tract **Management:** * Stroke treatment * Physical rehabilitation --- ### **9. Lateral Pontine Syndrome (AICA)** **Case Scenario:** Patient presents with facial paralysis, loss of pain and temperature on contralateral body, and vertigo. **Explanation:** AICA infarct affects: * Facial nerve * Spinothalamic tract * Vestibular nuclei **Management:** * Antiplatelets * Symptomatic vertigo treatment --- ### **10. Locked-In Syndrome** **Case Scenario:** Patient is conscious but cannot move limbs or speak, only vertical eye movements preserved. **Explanation:** Bilateral lesion of **ventral pons** * Corticospinal * Corticobulbar tracts **Management:** * Supportive ICU care * Communication aids * Prevention of complications --- ## **MEDULLARY SYNDROMES** --- ### **11. Lateral Medullary Syndrome (Wallenberg)** **Case Scenario:** Patient has dysphagia, hoarseness, ipsilateral facial pain loss, and contralateral body pain loss. **Explanation:** PICA infarct affects: * Nucleus ambiguus * Spinothalamic tract * Inferior cerebellar peduncle **Management:** * Airway protection * Nasogastric feeding * Stroke management --- ### **12. Medial Medullary Syndrome (Dejerine)** **Case Scenario:** Contralateral hemiplegia with loss of proprioception and ipsilateral tongue deviation. **Explanation:** Anterior spinal artery infarct involving: * Hypoglossal nerve * Corticospinal tract * Medial lemniscus **Management:** * Antiplatelets * Speech therapy --- ### **13. Jackson Syndrome** **Case Scenario:** Patient presents with ipsilateral hypoglossal paralysis and contralateral hemiplegia. **Explanation:** Lesion affects: * Hypoglossal nerve * Corticospinal tract **Management:** * Treat underlying lesion * Rehabilitation --- ### **14. Avellis Syndrome** **Case Scenario:** Hoarseness with contralateral loss of pain and temperature. **Explanation:** Lesion affects: * Nucleus ambiguus * Spinothalamic tract **Management:** * Swallowing therapy * Stroke care --- ### **15. Babinski-Nageotte Syndrome** **Case Scenario:** Features of lateral medullary syndrome plus contralateral hemiplegia. **Explanation:** Extension of lateral medullary lesion into corticospinal tract. **Management:** * Stroke management * Physiotherapy --- ## **MIXED AND FUNCTIONAL BRAINSTEM SYNDROMES** --- ### **16. Central Pontine Myelinolysis** **Case Scenario:** Alcoholic patient develops acute quadriplegia after rapid sodium correction. **Explanation:** Demyelination of central pons due to osmotic injury. **Management:** * Slow correction of sodium * Supportive care --- ### **17. Brainstem Glioma** **Case Scenario:** Child presents with cranial nerve palsies and long tract signs. **Explanation:** Diffuse intrinsic pontine glioma compresses nuclei. **Management:** * Radiotherapy * Steroids --- ### **18. Multiple Sclerosis Brainstem Lesion** **Case Scenario:** Young female with internuclear ophthalmoplegia and sensory symptoms. **Explanation:** Demyelination of medial longitudinal fasciculus. **Management:** * High-dose steroids * Disease-modifying therapy --- ### **19. Syringobulbia** **Case Scenario:** Patient has dissociated sensory loss in face with dysphagia. **Explanation:** Extension of syrinx into brainstem. **Management:** * Neurosurgical decompression --- ### **20. Brainstem Encephalitis** **Case Scenario:** Fever, altered sensorium, and multiple cranial nerve palsies. **Explanation:** Inflammatory involvement of brainstem nuclei. **Management:** * Antivirals or antibiotics * ICU monitoring --- ## **ADDITIONAL HIGH-YIELD CASE SCENARIOS** --- ### **21. Inferior Alternating Hemiplegia** **22. Superior Alternating Hemiplegia** **23. Pontine Hemorrhage** **24. Vertebrobasilar Insufficiency** **25. Brainstem Abscess** **26. Cavernous Hemangioma of Brainstem** **27. Progressive Bulbar Palsy** **28. Motor Neuron Disease with Brainstem Involvement** **29. Trauma-Induced Brainstem Lesion** **30. Metabolic Brainstem Dysfunction** *(Each presents with characteristic cranial nerve palsies + long tract signs and is managed by treating the underlying cause with supportive neurocritical care.)* --- ## **Key Exam Tip** > **Brainstem syndromes always show “crossed findings” – ipsilateral cranial nerve palsy with contralateral motor or sensory deficit.** --- ## **FAQ (SEO-Friendly)** **Q1. Which artery causes lateral medullary syndrome?** Posterior inferior cerebellar artery (PICA). **Q2. Most common brainstem stroke?** Lateral medullary syndrome. **Q3. Why is locked-in syndrome unique?** Consciousness preserved with complete paralysis. **Q4. Which nerve is involved in medial medullary syndrome?** Hypoglossal nerve. --- If you want, I can also provide: * **30 hard case-based MCQs** * **HTML/CSS/JS exam mode test** * **Schema-ready FAQ + breadcrumb** * **Illustrated lesion localization tables** Just tell me what to generate next.
Cerebellum Anatomy Structure Functions and Clinical Importance
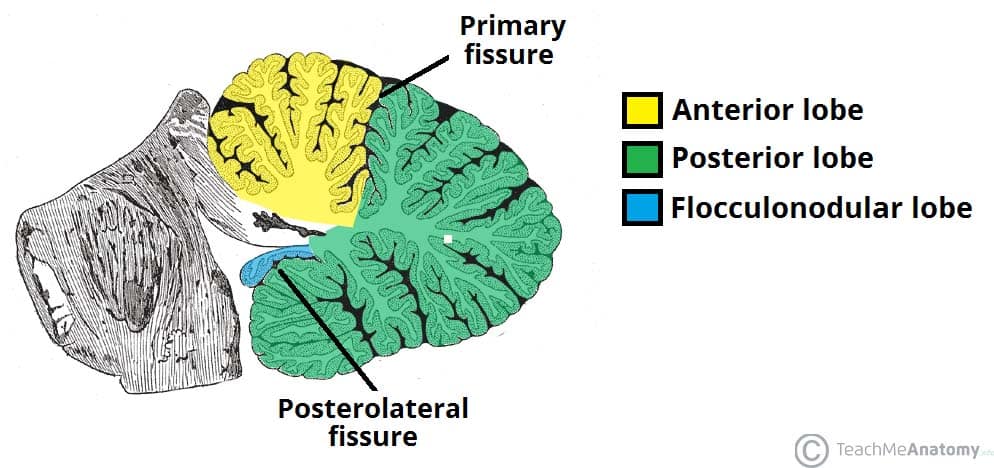
## Cerebellum Anatomy – Complete SEO-Friendly Guide ### Introduction The **cerebellum** is a major part of the hindbrain that plays a critical role in **coordination of movement, balance, posture, muscle tone, and motor learning**. Although it does not initiate movement, it fine-tunes motor activity to ensure accuracy and smooth execution. --- ## Location and Relations * Situated in the **posterior cranial fossa** * Lies **behind the pons and medulla** * Separated from the cerebrum by the **tentorium cerebelli** * Forms the **roof of the fourth ventricle** --- ## Gross Anatomy of the Cerebellum ### External Features The cerebellum consists of: 1. **Two hemispheres** (right and left) 2. **Vermis** (midline structure connecting hemispheres) #### Surfaces * **Superior surface** * **Inferior surface** * Both surfaces show numerous transverse folds called **folia** --- ## Lobes of the Cerebellum The cerebellum is divided by fissures into **three lobes**: ### 1. Anterior Lobe * Located anterior to the **primary fissure** * Functionally related to **spinocerebellum** * Involved in **posture and gait control** ### 2. Posterior Lobe * Largest lobe * Lies between primary fissure and posterolateral fissure * Involved in **fine voluntary movements** ### 3. Flocculonodular Lobe * Composed of **flocculus + nodulus** * Also called **vestibulocerebellum** * Responsible for **balance and eye movements** --- ## Functional Divisions of the Cerebellum ### 1. Cerebrocerebellum * Lateral hemispheres * Connected to cerebral cortex * Controls **planning and coordination of skilled movements** ### 2. Spinocerebellum * Vermis and intermediate zones * Regulates **muscle tone and ongoing movements** ### 3. Vestibulocerebellum * Flocculonodular lobe * Maintains **equilibrium and eye coordination** --- ## Cerebellar Cortex (Microscopic Anatomy) ### Layers of Cerebellar Cortex The cerebellar cortex has **three layers**: 1. **Molecular Layer** * Contains stellate and basket cells * Few neurons, mostly fibers 2. **Purkinje Cell Layer** * Single layer of large **Purkinje cells** * Output neurons of the cerebellar cortex * Inhibitory (GABAergic) 3. **Granular Layer** * Contains granule cells and Golgi cells * Highly cellular --- ## White Matter of Cerebellum * Located deep to the cortex * Appears as **arbor vitae** (tree-like pattern) * Carries fibers connecting cortex to cerebellar nuclei --- ## Deep Cerebellar Nuclei Embedded within white matter: 1. **Dentate** 2. **Emboliform** 3. **Globose** 4. **Fastigial** These nuclei serve as **major output centers** of the cerebellum. --- ## Cerebellar Peduncles The cerebellum connects to the brainstem via **three paired peduncles**: ### 1. Superior Cerebellar Peduncle * Connects to **midbrain** * Mainly **efferent (output)** fibers ### 2. Middle Cerebellar Peduncle * Connects to **pons** * Largest peduncle * Carries **afferent fibers from cerebral cortex** ### 3. Inferior Cerebellar Peduncle * Connects to **medulla** * Mixed afferent and efferent fibers --- ## Blood Supply of the Cerebellum * **Superior cerebellar artery (SCA)** * **Anterior inferior cerebellar artery (AICA)** * **Posterior inferior cerebellar artery (PICA)** All arise from the **vertebrobasilar system**. --- ## Functional Summary * Coordinates voluntary movements * Maintains posture and balance * Regulates muscle tone * Involved in motor learning and error correction --- ## Clinical Correlation (Brief) Lesions of the cerebellum lead to: * **Ataxia** * **Dysmetria** * **Intention tremor** * **Nystagmus** * **Hypotonia** * **Scanning speech** --- ## SEO Title **Cerebellum Anatomy Structure Functions and Clinical Importance** ## Meta Description Comprehensive SEO-friendly guide on cerebellum anatomy covering location lobes functional divisions cerebellar cortex peduncles blood supply and clinical significance. ## SEO Keywords cerebellum anatomy, cerebellar lobes, cerebellar cortex layers, cerebellar peduncles, deep cerebellar nuclei, cerebellum functions, hindbrain anatomy, neuroanatomy cerebellum --- If you want next: * **30 case-based cerebellar lesion scenarios** * **Hard MCQs with explanations** * **Clinical syndromes of cerebellar lesions** * **HTML/CSS/JS exam-mode MCQs** Just tell me 👍 Below are **high-yield clinical case scenarios of cerebellar lesions with clear diagnosis and management**, written in an **exam-oriented, clinical approach**. Concise but complete. --- ## 1. Midline (Vermis) Lesion – Truncal Ataxia **Case** A 45-year-old man with chronic alcohol use presents with inability to sit or stand without support. Limb movements are relatively normal. Gait is broad-based and staggering. **Clinical Diagnosis** Vermian cerebellar lesion (anterior lobe degeneration) **Key Features** * Truncal ataxia * Broad-based gait * Minimal limb ataxia **Management** * Treat underlying cause (alcohol cessation) * Thiamine supplementation * Physiotherapy for gait and balance * Fall-prevention measures --- ## 2. Cerebellar Hemisphere Lesion – Ipsilateral Limb Ataxia **Case** A 60-year-old man with hypertension presents with clumsiness of the right hand. Finger-nose test shows past pointing on the right. **Clinical Diagnosis** Right cerebellar hemisphere infarction **Key Features** * Ipsilateral limb ataxia * Dysmetria * Intention tremor **Management** * MRI brain to confirm stroke * Antiplatelet therapy * Blood pressure and risk factor control * Neurorehabilitation --- ## 3. Flocculonodular Lobe Lesion – Balance Disorder **Case** A child presents with frequent falls, vertigo, and abnormal eye movements. **Clinical Diagnosis** Vestibulocerebellar lesion **Key Features** * Nystagmus * Vertigo * Severe balance impairment **Management** * Treat underlying cause (tumor/infection) * Vestibular rehabilitation * Anti-vertigo medications (short term) --- ## 4. Acute Cerebellar Stroke **Case** A 70-year-old patient presents with sudden onset vertigo, vomiting, ataxia, and headache. **Clinical Diagnosis** Cerebellar infarction (PICA/AICA territory) **Management** * Emergency CT/MRI brain * Manage raised intracranial pressure * Antiplatelet or anticoagulation as indicated * Neurosurgical decompression if brainstem compression --- ## 5. Cerebellar Hemorrhage **Case** A hypertensive patient develops sudden headache, vomiting, and rapid deterioration of consciousness. **Clinical Diagnosis** Cerebellar hemorrhage **Management** * Immediate CT brain * Blood pressure control * Neurosurgical evacuation if large bleed * ICU monitoring --- ## 6. Alcoholic Cerebellar Degeneration **Case** A chronic alcoholic presents with progressive gait instability over months. **Clinical Diagnosis** Anterior cerebellar lobe degeneration **Management** * Alcohol abstinence * Nutritional rehabilitation * Thiamine and multivitamins * Long-term physiotherapy --- ## 7. Multiple Sclerosis with Cerebellar Involvement **Case** A young woman presents with intention tremor, scanning speech, and nystagmus. **Clinical Diagnosis** Cerebellar involvement in multiple sclerosis **Management** * MRI brain with contrast * Acute relapse: corticosteroids * Disease-modifying therapy * Speech and occupational therapy --- ## 8. Cerebellar Tumor (Medulloblastoma) **Case** A child presents with morning vomiting, headache, and gait ataxia. **Clinical Diagnosis** Midline cerebellar tumor (medulloblastoma) **Management** * MRI brain * Surgical excision * Radiotherapy and chemotherapy * Long-term neurodevelopmental follow-up --- ## 9. Cerebellar Abscess **Case** A patient with chronic otitis media presents with fever, headache, and ataxia. **Clinical Diagnosis** Cerebellar abscess **Management** * MRI with contrast * IV broad-spectrum antibiotics * Surgical drainage if indicated * Treat source of infection --- ## 10. Drug-Induced Cerebellar Toxicity **Case** A patient on phenytoin presents with nystagmus and ataxia. **Clinical Diagnosis** Drug-induced cerebellar dysfunction **Management** * Check drug levels * Stop or reduce offending drug * Supportive care * Monitor recovery --- ## 11. Paraneoplastic Cerebellar Degeneration **Case** A middle-aged woman presents with rapidly progressive ataxia; later found to have ovarian carcinoma. **Clinical Diagnosis** Paraneoplastic cerebellar degeneration **Management** * Treat underlying malignancy * Immunotherapy (steroids, IVIG) * Supportive rehabilitation --- ## 12. Cerebellar Ataxia in Hypothyroidism **Case** A patient presents with slow speech, unsteady gait, and fatigue. **Clinical Diagnosis** Metabolic cerebellar dysfunction **Management** * Thyroid function tests * Thyroxine replacement * Gradual neurological improvement --- ## 13. Arnold–Chiari Malformation **Case** A young adult presents with occipital headache worsened by coughing and gait imbalance. **Clinical Diagnosis** Chiari malformation affecting cerebellum **Management** * MRI brain and cervical spine * Neurosurgical decompression if symptomatic * Analgesia for headache --- ## 14. Post-Infectious Cerebellitis **Case** A child develops acute ataxia after viral illness. **Clinical Diagnosis** Acute cerebellitis **Management** * Usually self-limiting * Supportive care * Steroids if severe * Physiotherapy --- ## 15. Degenerative Spinocerebellar Ataxia **Case** Progressive ataxia with positive family history. **Clinical Diagnosis** Spinocerebellar degeneration **Management** * Genetic testing * Symptomatic treatment * Rehabilitation * Genetic counseling --- ### One-Line Exam Summary > **Cerebellar lesions produce ipsilateral signs and are managed by treating the cause, controlling complications, and long-term neurorehabilitation.** If you want next: * **30 hard case-based MCQs** * **HTML/CSS/JS interactive exam module** * **Cerebellar syndromes comparison table** * **SEO FAQ schema for cerebellar lesions** Just tell me.
Comments & Discussion
Use this thread like a mini viva: add differentials, staging systems, drug regimens and exam tricks.
Login or register to comment.
No comments yet – start by adding exam-style discussion points.