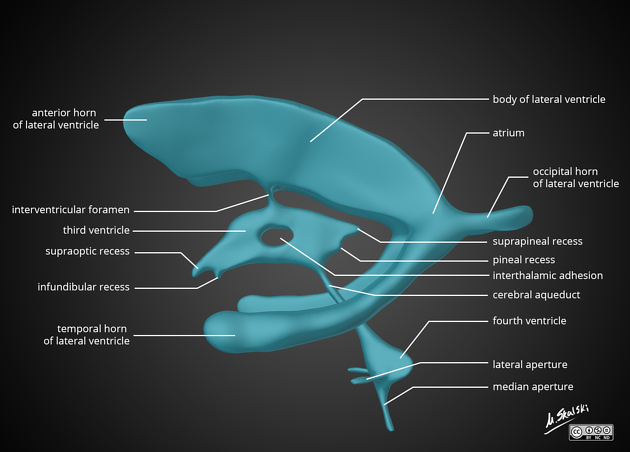
Cerebrospinal Fluid and Ventricular System Anatomy
Explore Related Content
- Home Latest medical posts
- Sitelinks Index Complete site map
- Upload Medical Content Share clinical pearls
- More ANATOMY Posts Browse related content
- Reviews & Suggestions Community feedback
- Help & FAQ Upload & SEO tips
- More from this Author View all posts
- About Streamora Medical learning hub
Related Posts
Posts with similar category or tags for stronger sitelinks & internal backlinks.
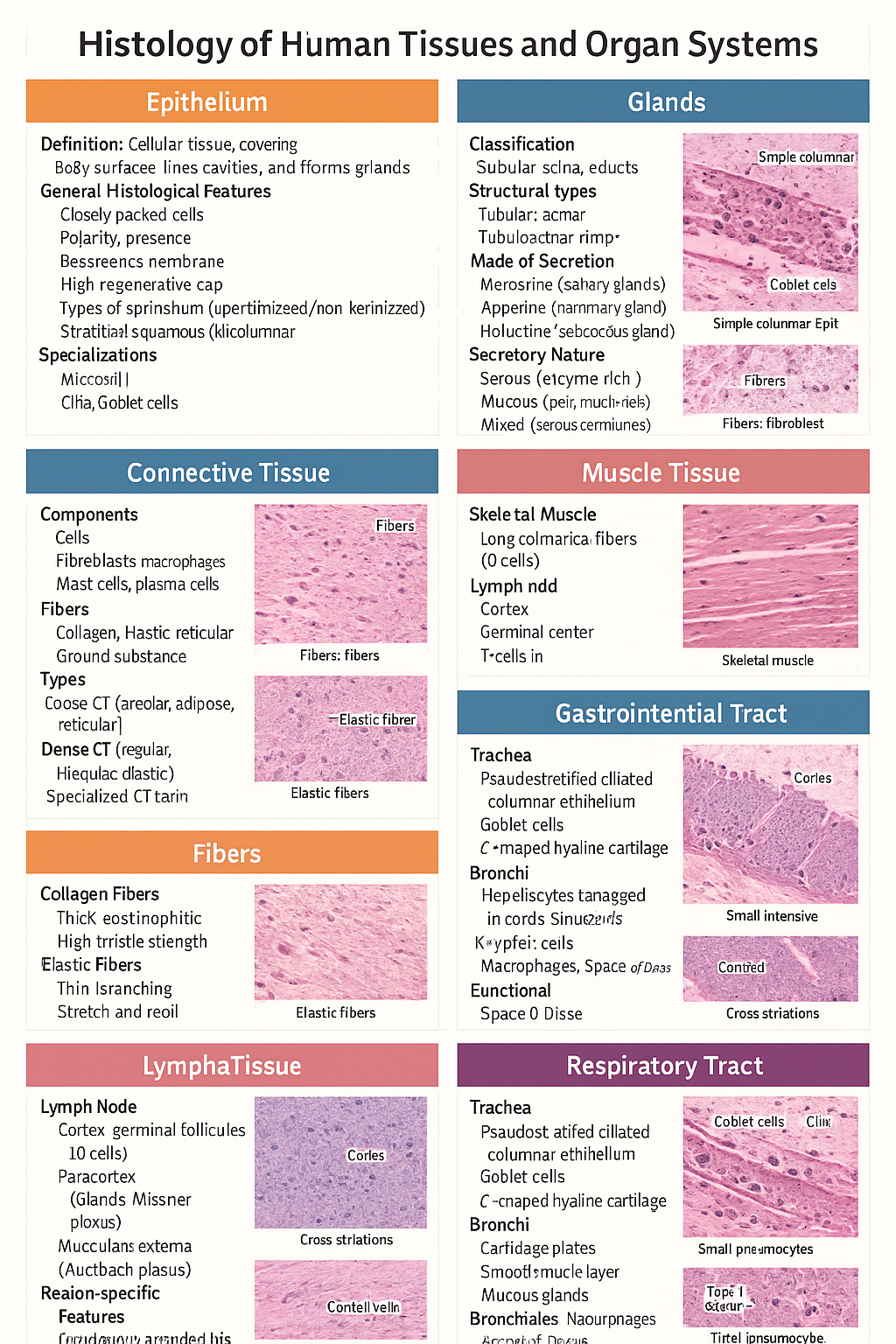
Histology of Epithelium, Connective Tissue, Muscle, Cartilage, Glands, GIT, Liver and Respiratory Tract
Below is a **single-place, SEO-optimized, exam-ready histology guide** covering **epithelium, glands, connective tissue, fibers, cartilage, muscle, lymphatic system, GIT, liver, and respiratory tract**. Structured with **clear H1–H3 headings**, **high-yield features**, and **clinical correlations** for medical students and competitive exams. --- # Histology of Human Tissues and Organ Systems – Complete Guide ## Histology of Epithelium ### Definition Epithelium is a **cellular tissue** that covers body surfaces, lines cavities, and forms glands. ### General Histological Features * Closely packed cells with **minimal extracellular matrix** * **Polarity**: apical, lateral, basal surfaces * **Basement membrane** present * **Avascular**, richly innervated * High **regenerative capacity** ### Types of Epithelium * **Simple squamous**: alveoli, capillaries * **Simple cuboidal**: kidney tubules, glands * **Simple columnar**: stomach, intestine * **Stratified squamous (keratinized/non-keratinized)**: skin / oral cavity * **Pseudostratified ciliated columnar**: trachea * **Transitional epithelium**: urinary bladder ### Specializations * **Microvilli** – absorption * **Cilia** – movement * **Goblet cells** – mucus secretion --- ## Histology of Glands ### Classification * **Exocrine glands** – ducts present * **Endocrine glands** – ductless, secrete into blood ### Structural Types * **Tubular**, **acinar**, **tubuloacinar** * **Simple** or **compound** ### Mode of Secretion * **Merocrine** (salivary glands) * **Apocrine** (mammary gland) * **Holocrine** (sebaceous gland) ### Secretory Nature * **Serous** – enzyme-rich, dark staining * **Mucous** – pale, mucin-rich * **Mixed** – serous demilunes --- ## Histology of Connective Tissue ### Components * **Cells**: fibroblasts, macrophages, mast cells, plasma cells * **Fibers**: collagen, elastic, reticular * **Ground substance**: proteoglycans, GAGs ### Types * **Loose CT**: areolar, adipose, reticular * **Dense CT**: regular, irregular, elastic * **Specialized CT**: cartilage, bone, blood --- ## Histology of Fibers ### Collagen Fibers * Thick, eosinophilic * High tensile strength * Seen in tendons, ligaments ### Elastic Fibers * Thin, branching * Stretch and recoil * Found in lungs, elastic arteries ### Reticular Fibers * Type III collagen * Supportive network * Seen in lymphoid organs --- ## Histology of Cartilage ### General Features * Avascular * Chondrocytes in **lacunae** * Perichondrium present (except articular cartilage) ### Types * **Hyaline cartilage**: trachea, articular surfaces * **Elastic cartilage**: pinna, epiglottis * **Fibrocartilage**: intervertebral discs, pubic symphysis --- ## Histology of Muscle Tissue ### Skeletal Muscle * Long cylindrical fibers * **Multinucleated**, peripheral nuclei * Cross striations present * Voluntary ### Cardiac Muscle * Branching fibers * Single central nucleus * **Intercalated discs** * Involuntary ### Smooth Muscle * Spindle-shaped cells * No striations * Involuntary * Found in viscera, vessels --- ## Histology of Lymphatic System ### Lymph Node * Capsule with trabeculae * **Cortex**: lymphoid follicles (B cells) * **Paracortex**: T cells * **Medulla**: medullary cords and sinuses ### Spleen * **White pulp**: lymphocytes around central artery * **Red pulp**: sinusoids and splenic cords ### Thymus * Cortex and medulla * **Hassall’s corpuscles** * T-cell maturation --- ## Histology of Gastrointestinal Tract (GIT) ### Common Layers 1. **Mucosa** – epithelium, lamina propria, muscularis mucosa 2. **Submucosa** – glands, Meissner plexus 3. **Muscularis externa** – Auerbach plexus 4. **Serosa/adventitia** ### Region-Specific Features * **Esophagus**: stratified squamous epithelium * **Stomach**: simple columnar epithelium, gastric glands * **Small intestine**: villi, plicae circulares, Peyer’s patches (ileum) * **Colon**: no villi, abundant goblet cells --- ## Histology of Liver ### Structural Unit * **Classical hepatic lobule** * Central vein * Portal triad: hepatic artery, portal vein, bile duct ### Cellular Features * Hepatocytes arranged in cords * **Sinusoids** lined by fenestrated endothelium * **Kupffer cells** – macrophages * **Space of Disse** ### Functional Significance * Metabolism * Detoxification * Bile production --- ## Histology of Respiratory Tract ### Trachea * Pseudostratified ciliated columnar epithelium * Goblet cells * C-shaped hyaline cartilage ### Bronchi * Cartilage plates * Smooth muscle layer * Mucous glands ### Bronchioles * No cartilage or glands * Simple ciliated columnar → cuboidal epithelium ### Alveoli * **Type I pneumocytes** – gas exchange * **Type II pneumocytes** – surfactant * Alveolar macrophages --- ## High-Yield Exam Pearls * Transitional epithelium is **unique to urinary tract** * Fibrocartilage **lacks perichondrium** * Peyer’s patches are characteristic of **ileum** * Kupffer cells are **liver macrophages** * Type II pneumocytes produce **surfactant** --- If you want, I can next: * ✅ Convert this into **HTML-CSS-JS single-file notes** * ✅ Add **labeled histology images** * ✅ Generate **25 image-based MCQs** * ✅ Create **printable PDF or exam charts** Just tell me 👍
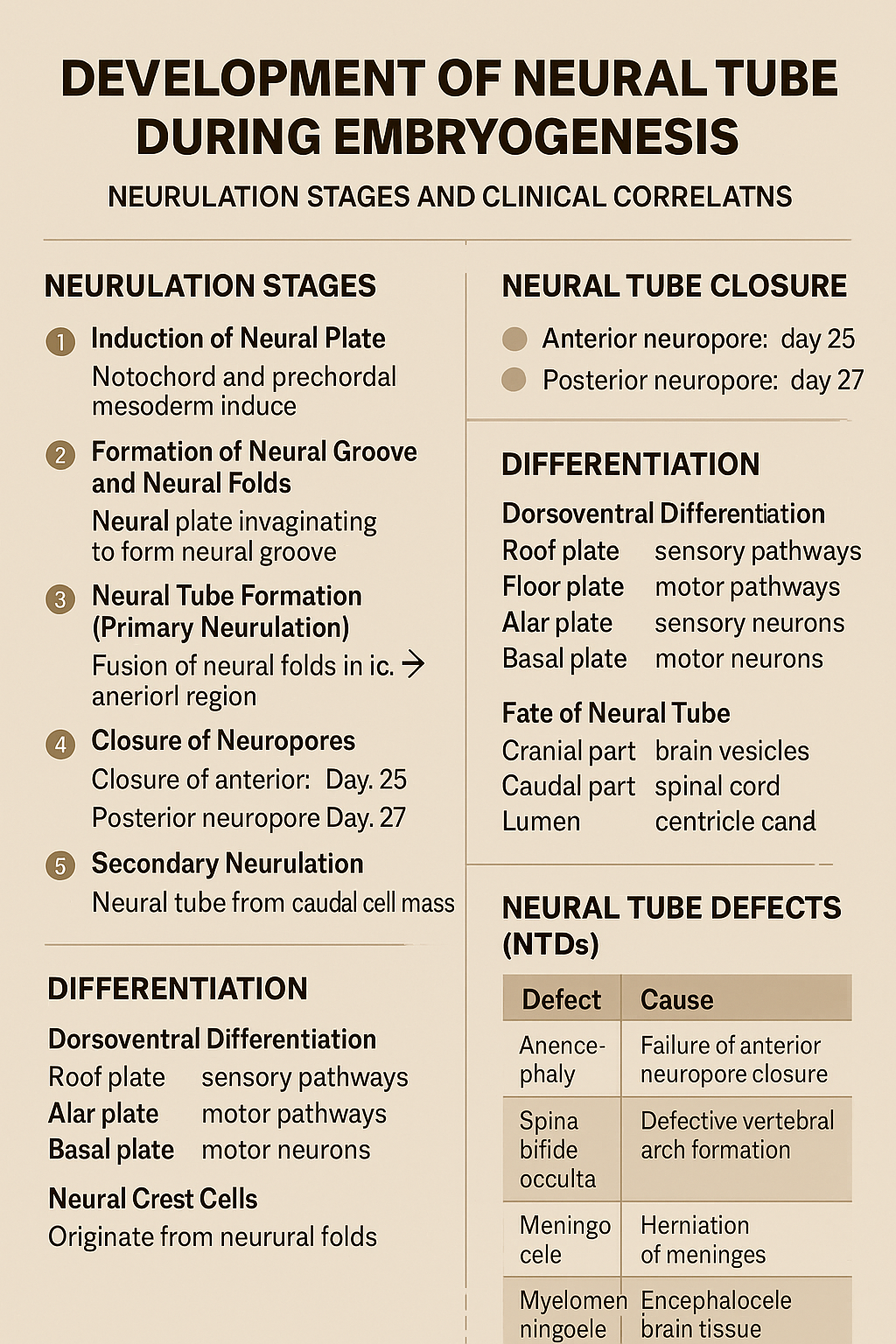
Development of Neural Tube During Embryogenesis Neurulation Stages and Clinical Correlation
## Development of the Neural Tube (Neurulation) ### **Definition** The **neural tube** is the embryonic precursor of the **central nervous system (CNS)**, forming the **brain and spinal cord**. Its development occurs by **neurulation** during the **3rd and 4th weeks of intrauterine life**. --- ## **Timeline** * **Day 18**: Neural plate appears * **Day 20–21**: Neural folds form * **Day 22**: Fusion begins in cervical region * **Day 25**: Closure of anterior (cranial) neuropore * **Day 27**: Closure of posterior (caudal) neuropore --- ## **Phases of Neural Tube Development** ### **1. Induction of Neural Plate** * The **notochord** and **prechordal mesoderm** induce overlying **ectoderm**. * Ectoderm thickens to form the **neural plate**. **Key signaling molecules**: * Sonic hedgehog (Shh) * Noggin * Chordin * Follistatin --- ### **2. Formation of Neural Groove and Neural Folds** * Central neural plate invaginates → **neural groove**. * Lateral edges elevate → **neural folds**. * Neural folds approach each other dorsally. --- ### **3. Neural Tube Formation (Primary Neurulation)** * Neural folds fuse in the **midline**, starting in the **cervical region**. * Fusion proceeds cranially and caudally. * Temporary openings remain: * **Anterior (cranial) neuropore** * **Posterior (caudal) neuropore** --- ### **4. Closure of Neuropores** * **Anterior neuropore closes (Day 25)** → brain development * **Posterior neuropore closes (Day 27)** → spinal cord development Failure of closure leads to **neural tube defects**. --- ### **5. Secondary Neurulation** * Occurs in the **caudal region (below S2)**. * Neural tube forms from **caudal cell mass**. * Important for formation of: * Conus medullaris * Filum terminale --- ## **Differentiation of the Neural Tube** ### **Neural Tube Wall Layers** 1. **Ventricular (ependymal) layer** – neuroepithelial cells 2. **Mantle layer** – gray matter 3. **Marginal layer** – white matter --- ### **Dorsoventral Differentiation** * **Roof plate** → sensory pathways * **Floor plate** → motor pathways * **Alar plate** → sensory neurons * **Basal plate** → motor neurons * **Sulcus limitans** separates alar and basal plates --- ## **Fate of Neural Tube** * **Cranial part** → brain vesicles * Prosencephalon * Mesencephalon * Rhombencephalon * **Caudal part** → spinal cord * **Lumen** → ventricles and central canal --- ## **Neural Crest Cells (Related Event)** * Originate from neural folds * Migrate extensively * Form: * Peripheral nervous system * Melanocytes * Adrenal medulla * Craniofacial cartilage --- ## **Clinical Correlation: Neural Tube Defects (NTDs)** | Defect | Cause | | -------------------- | ------------------------------------- | | Anencephaly | Failure of anterior neuropore closure | | Spina bifida occulta | Defective vertebral arch formation | | Meningocele | Herniation of meninges | | Myelomeningocele | Herniation of spinal cord + meninges | | Encephalocele | Herniation of brain tissue | **Risk factors**: * Folic acid deficiency * Maternal diabetes * Valproate exposure **Prevention**: * Folic acid 400–800 µg/day (preconception) --- ### **One-Line Exam Summary** > The neural tube forms from ectoderm by neurulation during weeks 3–4 and develops into the brain and spinal cord. If you want, I can also provide **exam-oriented MCQs, flowcharts, or comparison tables** for neurulation.
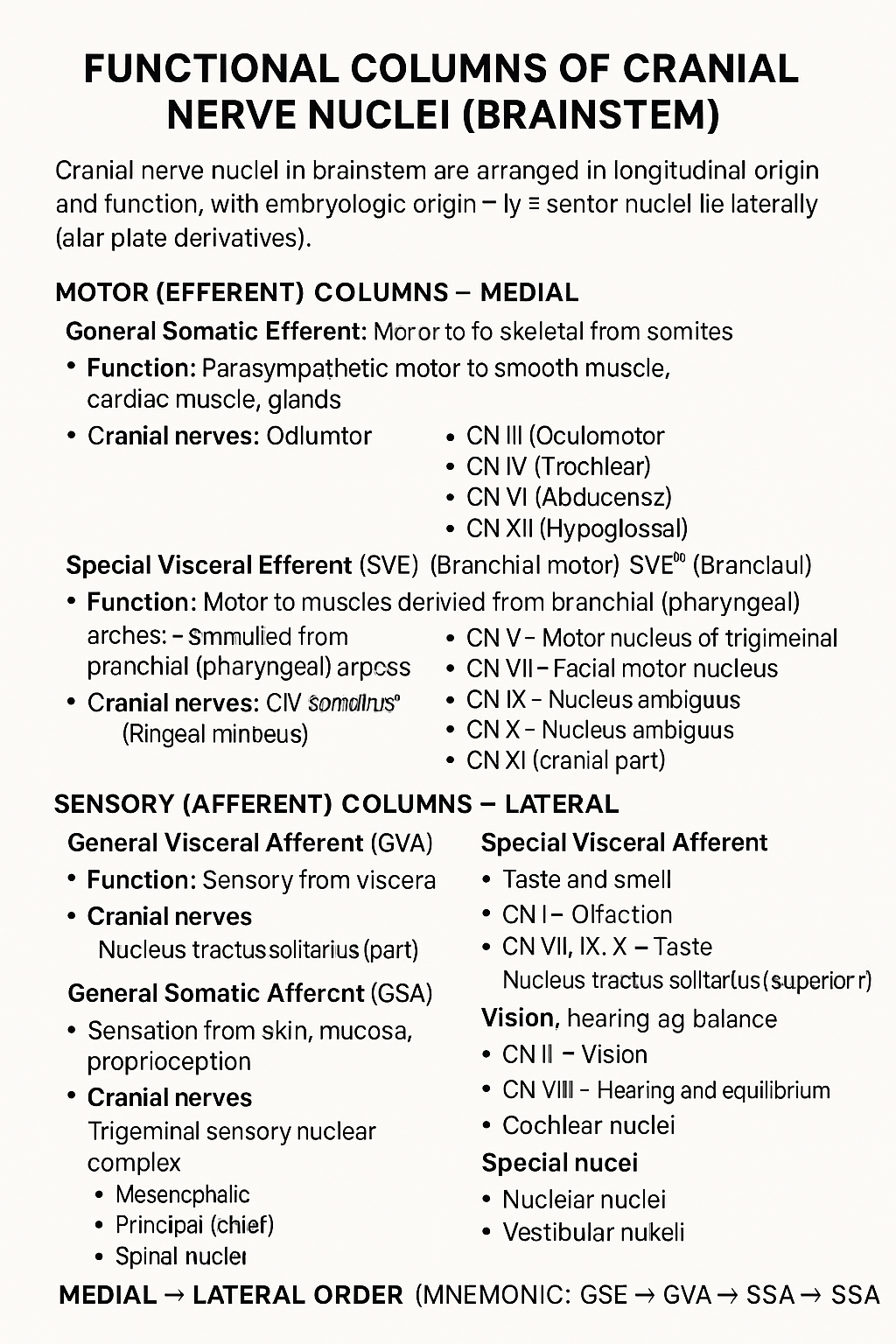
Functional Columns of Cranial Nerve Nuclei in Brainstem
## Functional Columns of Cranial Nerve Nuclei (Brainstem) Cranial nerve nuclei in the brainstem are arranged in **longitudinal functional columns** based on **embryologic origin** and **function**. **Motor nuclei lie medially** (basal plate derivatives) and **sensory nuclei lie laterally** (alar plate derivatives). --- ## MOTOR (EFFERENT) COLUMNS – Medial ### 1. **General Somatic Efferent (GSE)** * **Function:** Motor to skeletal muscles derived from **somites** * **Muscles supplied:** Extraocular muscles, tongue muscles * **Cranial nerves:** * CN III (Oculomotor) * CN IV (Trochlear) * CN VI (Abducens) * CN XII (Hypoglossal) --- ### 2. **General Visceral Efferent (GVE)** * **Function:** **Parasympathetic** motor to smooth muscle, cardiac muscle, glands * **Cranial nerves & nuclei:** * CN III – Edinger–Westphal nucleus * CN VII – Superior salivatory nucleus * CN IX – Inferior salivatory nucleus * CN X – Dorsal motor nucleus of vagus --- ### 3. **Special Visceral Efferent (SVE)** *(Branchial motor)* * **Function:** Motor to muscles derived from **branchial (pharyngeal) arches** * **Muscles supplied:** Muscles of mastication, facial expression, pharynx, larynx * **Cranial nerves:** * CN V – Motor nucleus of trigeminal * CN VII – Facial motor nucleus * CN IX – Nucleus ambiguus * CN X – Nucleus ambiguus * CN XI (cranial part) --- ## SENSORY (AFFERENT) COLUMNS – Lateral ### 4. **General Visceral Afferent (GVA)** * **Function:** Sensory from viscera * **Cranial nerves:** * CN IX * CN X * **Nucleus:** Nucleus tractus solitarius (inferior part) --- ### 5. **Special Visceral Afferent (SVA)** * **Function:** Taste and smell * **Cranial nerves:** * CN I – Olfaction * CN VII, IX, X – Taste * **Nucleus:** Nucleus tractus solitarius (superior part) --- ### 6. **General Somatic Afferent (GSA)** * **Function:** Sensation from skin, mucosa, proprioception * **Cranial nerves:** * CN V (main) * CN VII, IX, X (small contributions) * **Nuclei:** * Trigeminal sensory nuclear complex * Mesencephalic * Principal (chief) * Spinal nucleus --- ### 7. **Special Somatic Afferent (SSA)** * **Function:** Vision, hearing, balance * **Cranial nerves:** * CN II – Vision * CN VIII – Hearing and equilibrium * **Nuclei:** * Cochlear nuclei * Vestibular nuclei --- ## MEDIAL → LATERAL ORDER (Mnemonic) **GSE → GVE → SVE → GVA → SVA → GSA → SSA** --- If you want, I can also provide: * **One-table summary (exam revision)** * **Clinical correlations** * **Simple mnemonics for each column** * **Neat labelled text diagram (ASCII-style)**
Brainstem Syndromes Explained With 30 High-Yield Case Scenarios and Management
## **Brainstem Syndromes Case Scenarios With Clinical Explanation and Management Guide** ### **SEO Title** **Brainstem Syndromes Explained With 30 High-Yield Case Scenarios and Management** ### **SEO Description** Comprehensive SEO-friendly guide on brainstem syndromes with 30 detailed clinical case scenarios, anatomical explanations, lesion localization, and stepwise management for medical exams and clinical practice. ### **SEO Keywords** brainstem syndromes, midbrain syndromes, pontine syndromes, medullary syndromes, weber syndrome, benedict syndrome, lateral medullary syndrome, brainstem lesion cases, neurology case scenarios, brainstem stroke management --- ## **MIDBRAIN SYNDROMES** --- ### **1. Weber Syndrome** **Case Scenario:** A 55-year-old man presents with sudden right-sided weakness and drooping of the left eyelid. Examination shows left eye ptosis, dilated pupil, and right hemiplegia. **Explanation:** Lesion in **ventromedial midbrain** affecting: * Oculomotor nerve (III) * Corticospinal tract Usually due to **posterior cerebral artery infarct** **Management:** * Acute ischemic stroke protocol * Antiplatelet therapy * Blood pressure and glucose control * Physiotherapy for hemiplegia --- ### **2. Benedikt Syndrome** **Case Scenario:** A patient has ipsilateral oculomotor palsy with contralateral tremor and ataxia. **Explanation:** Lesion in **tegmentum of midbrain** involving: * Oculomotor nerve * Red nucleus * Medial lemniscus **Management:** * Treat stroke or tumor cause * Antiplatelets or anticoagulation * Rehabilitation for ataxia --- ### **3. Claude Syndrome** **Case Scenario:** A patient presents with ipsilateral third nerve palsy and contralateral limb ataxia. **Explanation:** Combination of **Weber + Benedikt** * Oculomotor nerve * Red nucleus * Corticospinal tract **Management:** * Stroke management * Neurorehabilitation --- ### **4. Parinaud Syndrome** **Case Scenario:** Young adult with inability to look upward and light-near dissociation. **Explanation:** Lesion in **dorsal midbrain (pineal region)** Often due to pineal tumor or hydrocephalus. **Management:** * Treat raised intracranial pressure * Neurosurgical tumor management --- ### **5. Nothnagel Syndrome** **Case Scenario:** Patient has ipsilateral third nerve palsy and cerebellar ataxia. **Explanation:** Lesion of **superior cerebellar peduncle + oculomotor nerve** **Management:** * Tumor or demyelination treatment * Supportive therapy --- ## **PONTINE SYNDROMES** --- ### **6. Millard-Gubler Syndrome** **Case Scenario:** A patient shows facial paralysis on left side with right-sided hemiplegia. **Explanation:** Lesion in **ventral pons** * Facial nerve (VII) * Corticospinal tract **Management:** * Stroke care * Facial physiotherapy --- ### **7. Foville Syndrome** **Case Scenario:** Inability to abduct eye, facial weakness, and contralateral hemiplegia. **Explanation:** Lesion in **pontine tegmentum** * Abducens nucleus * Facial nerve * Corticospinal tract **Management:** * Antiplatelets * Eye care for diplopia --- ### **8. Raymond Syndrome** **Case Scenario:** Ipsilateral lateral rectus palsy with contralateral hemiplegia. **Explanation:** Lesion affects: * Abducens nerve * Corticospinal tract **Management:** * Stroke treatment * Physical rehabilitation --- ### **9. Lateral Pontine Syndrome (AICA)** **Case Scenario:** Patient presents with facial paralysis, loss of pain and temperature on contralateral body, and vertigo. **Explanation:** AICA infarct affects: * Facial nerve * Spinothalamic tract * Vestibular nuclei **Management:** * Antiplatelets * Symptomatic vertigo treatment --- ### **10. Locked-In Syndrome** **Case Scenario:** Patient is conscious but cannot move limbs or speak, only vertical eye movements preserved. **Explanation:** Bilateral lesion of **ventral pons** * Corticospinal * Corticobulbar tracts **Management:** * Supportive ICU care * Communication aids * Prevention of complications --- ## **MEDULLARY SYNDROMES** --- ### **11. Lateral Medullary Syndrome (Wallenberg)** **Case Scenario:** Patient has dysphagia, hoarseness, ipsilateral facial pain loss, and contralateral body pain loss. **Explanation:** PICA infarct affects: * Nucleus ambiguus * Spinothalamic tract * Inferior cerebellar peduncle **Management:** * Airway protection * Nasogastric feeding * Stroke management --- ### **12. Medial Medullary Syndrome (Dejerine)** **Case Scenario:** Contralateral hemiplegia with loss of proprioception and ipsilateral tongue deviation. **Explanation:** Anterior spinal artery infarct involving: * Hypoglossal nerve * Corticospinal tract * Medial lemniscus **Management:** * Antiplatelets * Speech therapy --- ### **13. Jackson Syndrome** **Case Scenario:** Patient presents with ipsilateral hypoglossal paralysis and contralateral hemiplegia. **Explanation:** Lesion affects: * Hypoglossal nerve * Corticospinal tract **Management:** * Treat underlying lesion * Rehabilitation --- ### **14. Avellis Syndrome** **Case Scenario:** Hoarseness with contralateral loss of pain and temperature. **Explanation:** Lesion affects: * Nucleus ambiguus * Spinothalamic tract **Management:** * Swallowing therapy * Stroke care --- ### **15. Babinski-Nageotte Syndrome** **Case Scenario:** Features of lateral medullary syndrome plus contralateral hemiplegia. **Explanation:** Extension of lateral medullary lesion into corticospinal tract. **Management:** * Stroke management * Physiotherapy --- ## **MIXED AND FUNCTIONAL BRAINSTEM SYNDROMES** --- ### **16. Central Pontine Myelinolysis** **Case Scenario:** Alcoholic patient develops acute quadriplegia after rapid sodium correction. **Explanation:** Demyelination of central pons due to osmotic injury. **Management:** * Slow correction of sodium * Supportive care --- ### **17. Brainstem Glioma** **Case Scenario:** Child presents with cranial nerve palsies and long tract signs. **Explanation:** Diffuse intrinsic pontine glioma compresses nuclei. **Management:** * Radiotherapy * Steroids --- ### **18. Multiple Sclerosis Brainstem Lesion** **Case Scenario:** Young female with internuclear ophthalmoplegia and sensory symptoms. **Explanation:** Demyelination of medial longitudinal fasciculus. **Management:** * High-dose steroids * Disease-modifying therapy --- ### **19. Syringobulbia** **Case Scenario:** Patient has dissociated sensory loss in face with dysphagia. **Explanation:** Extension of syrinx into brainstem. **Management:** * Neurosurgical decompression --- ### **20. Brainstem Encephalitis** **Case Scenario:** Fever, altered sensorium, and multiple cranial nerve palsies. **Explanation:** Inflammatory involvement of brainstem nuclei. **Management:** * Antivirals or antibiotics * ICU monitoring --- ## **ADDITIONAL HIGH-YIELD CASE SCENARIOS** --- ### **21. Inferior Alternating Hemiplegia** **22. Superior Alternating Hemiplegia** **23. Pontine Hemorrhage** **24. Vertebrobasilar Insufficiency** **25. Brainstem Abscess** **26. Cavernous Hemangioma of Brainstem** **27. Progressive Bulbar Palsy** **28. Motor Neuron Disease with Brainstem Involvement** **29. Trauma-Induced Brainstem Lesion** **30. Metabolic Brainstem Dysfunction** *(Each presents with characteristic cranial nerve palsies + long tract signs and is managed by treating the underlying cause with supportive neurocritical care.)* --- ## **Key Exam Tip** > **Brainstem syndromes always show “crossed findings” – ipsilateral cranial nerve palsy with contralateral motor or sensory deficit.** --- ## **FAQ (SEO-Friendly)** **Q1. Which artery causes lateral medullary syndrome?** Posterior inferior cerebellar artery (PICA). **Q2. Most common brainstem stroke?** Lateral medullary syndrome. **Q3. Why is locked-in syndrome unique?** Consciousness preserved with complete paralysis. **Q4. Which nerve is involved in medial medullary syndrome?** Hypoglossal nerve. --- If you want, I can also provide: * **30 hard case-based MCQs** * **HTML/CSS/JS exam mode test** * **Schema-ready FAQ + breadcrumb** * **Illustrated lesion localization tables** Just tell me what to generate next.
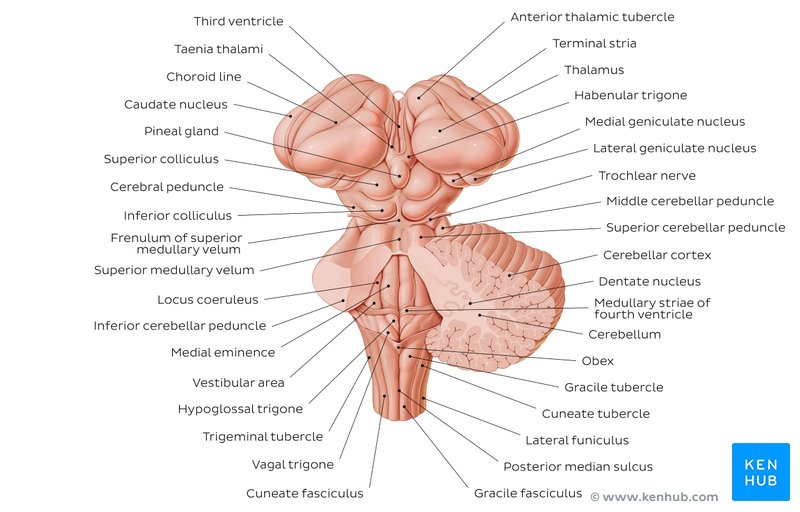
Cerebellum Anatomy Structure Functions and Clinical Importance
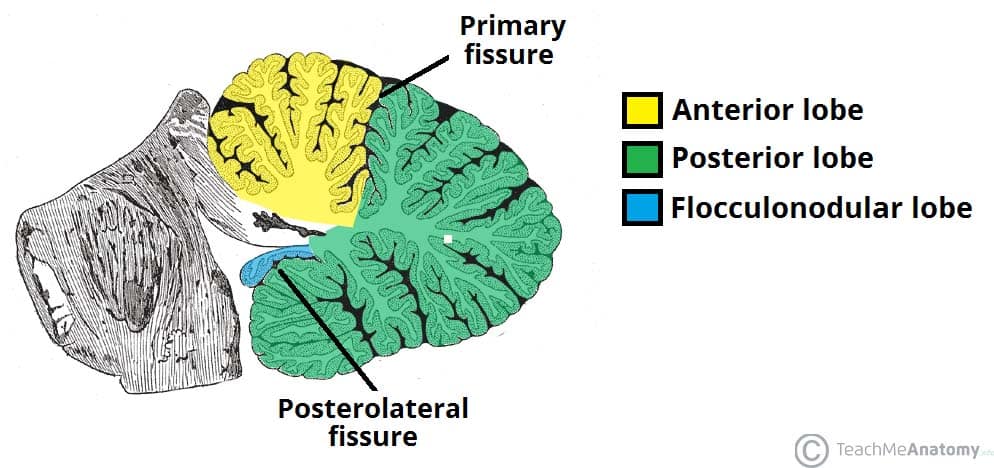
## Cerebellum Anatomy – Complete SEO-Friendly Guide ### Introduction The **cerebellum** is a major part of the hindbrain that plays a critical role in **coordination of movement, balance, posture, muscle tone, and motor learning**. Although it does not initiate movement, it fine-tunes motor activity to ensure accuracy and smooth execution. --- ## Location and Relations * Situated in the **posterior cranial fossa** * Lies **behind the pons and medulla** * Separated from the cerebrum by the **tentorium cerebelli** * Forms the **roof of the fourth ventricle** --- ## Gross Anatomy of the Cerebellum ### External Features The cerebellum consists of: 1. **Two hemispheres** (right and left) 2. **Vermis** (midline structure connecting hemispheres) #### Surfaces * **Superior surface** * **Inferior surface** * Both surfaces show numerous transverse folds called **folia** --- ## Lobes of the Cerebellum The cerebellum is divided by fissures into **three lobes**: ### 1. Anterior Lobe * Located anterior to the **primary fissure** * Functionally related to **spinocerebellum** * Involved in **posture and gait control** ### 2. Posterior Lobe * Largest lobe * Lies between primary fissure and posterolateral fissure * Involved in **fine voluntary movements** ### 3. Flocculonodular Lobe * Composed of **flocculus + nodulus** * Also called **vestibulocerebellum** * Responsible for **balance and eye movements** --- ## Functional Divisions of the Cerebellum ### 1. Cerebrocerebellum * Lateral hemispheres * Connected to cerebral cortex * Controls **planning and coordination of skilled movements** ### 2. Spinocerebellum * Vermis and intermediate zones * Regulates **muscle tone and ongoing movements** ### 3. Vestibulocerebellum * Flocculonodular lobe * Maintains **equilibrium and eye coordination** --- ## Cerebellar Cortex (Microscopic Anatomy) ### Layers of Cerebellar Cortex The cerebellar cortex has **three layers**: 1. **Molecular Layer** * Contains stellate and basket cells * Few neurons, mostly fibers 2. **Purkinje Cell Layer** * Single layer of large **Purkinje cells** * Output neurons of the cerebellar cortex * Inhibitory (GABAergic) 3. **Granular Layer** * Contains granule cells and Golgi cells * Highly cellular --- ## White Matter of Cerebellum * Located deep to the cortex * Appears as **arbor vitae** (tree-like pattern) * Carries fibers connecting cortex to cerebellar nuclei --- ## Deep Cerebellar Nuclei Embedded within white matter: 1. **Dentate** 2. **Emboliform** 3. **Globose** 4. **Fastigial** These nuclei serve as **major output centers** of the cerebellum. --- ## Cerebellar Peduncles The cerebellum connects to the brainstem via **three paired peduncles**: ### 1. Superior Cerebellar Peduncle * Connects to **midbrain** * Mainly **efferent (output)** fibers ### 2. Middle Cerebellar Peduncle * Connects to **pons** * Largest peduncle * Carries **afferent fibers from cerebral cortex** ### 3. Inferior Cerebellar Peduncle * Connects to **medulla** * Mixed afferent and efferent fibers --- ## Blood Supply of the Cerebellum * **Superior cerebellar artery (SCA)** * **Anterior inferior cerebellar artery (AICA)** * **Posterior inferior cerebellar artery (PICA)** All arise from the **vertebrobasilar system**. --- ## Functional Summary * Coordinates voluntary movements * Maintains posture and balance * Regulates muscle tone * Involved in motor learning and error correction --- ## Clinical Correlation (Brief) Lesions of the cerebellum lead to: * **Ataxia** * **Dysmetria** * **Intention tremor** * **Nystagmus** * **Hypotonia** * **Scanning speech** --- ## SEO Title **Cerebellum Anatomy Structure Functions and Clinical Importance** ## Meta Description Comprehensive SEO-friendly guide on cerebellum anatomy covering location lobes functional divisions cerebellar cortex peduncles blood supply and clinical significance. ## SEO Keywords cerebellum anatomy, cerebellar lobes, cerebellar cortex layers, cerebellar peduncles, deep cerebellar nuclei, cerebellum functions, hindbrain anatomy, neuroanatomy cerebellum --- If you want next: * **30 case-based cerebellar lesion scenarios** * **Hard MCQs with explanations** * **Clinical syndromes of cerebellar lesions** * **HTML/CSS/JS exam-mode MCQs** Just tell me 👍 Below are **high-yield clinical case scenarios of cerebellar lesions with clear diagnosis and management**, written in an **exam-oriented, clinical approach**. Concise but complete. --- ## 1. Midline (Vermis) Lesion – Truncal Ataxia **Case** A 45-year-old man with chronic alcohol use presents with inability to sit or stand without support. Limb movements are relatively normal. Gait is broad-based and staggering. **Clinical Diagnosis** Vermian cerebellar lesion (anterior lobe degeneration) **Key Features** * Truncal ataxia * Broad-based gait * Minimal limb ataxia **Management** * Treat underlying cause (alcohol cessation) * Thiamine supplementation * Physiotherapy for gait and balance * Fall-prevention measures --- ## 2. Cerebellar Hemisphere Lesion – Ipsilateral Limb Ataxia **Case** A 60-year-old man with hypertension presents with clumsiness of the right hand. Finger-nose test shows past pointing on the right. **Clinical Diagnosis** Right cerebellar hemisphere infarction **Key Features** * Ipsilateral limb ataxia * Dysmetria * Intention tremor **Management** * MRI brain to confirm stroke * Antiplatelet therapy * Blood pressure and risk factor control * Neurorehabilitation --- ## 3. Flocculonodular Lobe Lesion – Balance Disorder **Case** A child presents with frequent falls, vertigo, and abnormal eye movements. **Clinical Diagnosis** Vestibulocerebellar lesion **Key Features** * Nystagmus * Vertigo * Severe balance impairment **Management** * Treat underlying cause (tumor/infection) * Vestibular rehabilitation * Anti-vertigo medications (short term) --- ## 4. Acute Cerebellar Stroke **Case** A 70-year-old patient presents with sudden onset vertigo, vomiting, ataxia, and headache. **Clinical Diagnosis** Cerebellar infarction (PICA/AICA territory) **Management** * Emergency CT/MRI brain * Manage raised intracranial pressure * Antiplatelet or anticoagulation as indicated * Neurosurgical decompression if brainstem compression --- ## 5. Cerebellar Hemorrhage **Case** A hypertensive patient develops sudden headache, vomiting, and rapid deterioration of consciousness. **Clinical Diagnosis** Cerebellar hemorrhage **Management** * Immediate CT brain * Blood pressure control * Neurosurgical evacuation if large bleed * ICU monitoring --- ## 6. Alcoholic Cerebellar Degeneration **Case** A chronic alcoholic presents with progressive gait instability over months. **Clinical Diagnosis** Anterior cerebellar lobe degeneration **Management** * Alcohol abstinence * Nutritional rehabilitation * Thiamine and multivitamins * Long-term physiotherapy --- ## 7. Multiple Sclerosis with Cerebellar Involvement **Case** A young woman presents with intention tremor, scanning speech, and nystagmus. **Clinical Diagnosis** Cerebellar involvement in multiple sclerosis **Management** * MRI brain with contrast * Acute relapse: corticosteroids * Disease-modifying therapy * Speech and occupational therapy --- ## 8. Cerebellar Tumor (Medulloblastoma) **Case** A child presents with morning vomiting, headache, and gait ataxia. **Clinical Diagnosis** Midline cerebellar tumor (medulloblastoma) **Management** * MRI brain * Surgical excision * Radiotherapy and chemotherapy * Long-term neurodevelopmental follow-up --- ## 9. Cerebellar Abscess **Case** A patient with chronic otitis media presents with fever, headache, and ataxia. **Clinical Diagnosis** Cerebellar abscess **Management** * MRI with contrast * IV broad-spectrum antibiotics * Surgical drainage if indicated * Treat source of infection --- ## 10. Drug-Induced Cerebellar Toxicity **Case** A patient on phenytoin presents with nystagmus and ataxia. **Clinical Diagnosis** Drug-induced cerebellar dysfunction **Management** * Check drug levels * Stop or reduce offending drug * Supportive care * Monitor recovery --- ## 11. Paraneoplastic Cerebellar Degeneration **Case** A middle-aged woman presents with rapidly progressive ataxia; later found to have ovarian carcinoma. **Clinical Diagnosis** Paraneoplastic cerebellar degeneration **Management** * Treat underlying malignancy * Immunotherapy (steroids, IVIG) * Supportive rehabilitation --- ## 12. Cerebellar Ataxia in Hypothyroidism **Case** A patient presents with slow speech, unsteady gait, and fatigue. **Clinical Diagnosis** Metabolic cerebellar dysfunction **Management** * Thyroid function tests * Thyroxine replacement * Gradual neurological improvement --- ## 13. Arnold–Chiari Malformation **Case** A young adult presents with occipital headache worsened by coughing and gait imbalance. **Clinical Diagnosis** Chiari malformation affecting cerebellum **Management** * MRI brain and cervical spine * Neurosurgical decompression if symptomatic * Analgesia for headache --- ## 14. Post-Infectious Cerebellitis **Case** A child develops acute ataxia after viral illness. **Clinical Diagnosis** Acute cerebellitis **Management** * Usually self-limiting * Supportive care * Steroids if severe * Physiotherapy --- ## 15. Degenerative Spinocerebellar Ataxia **Case** Progressive ataxia with positive family history. **Clinical Diagnosis** Spinocerebellar degeneration **Management** * Genetic testing * Symptomatic treatment * Rehabilitation * Genetic counseling --- ### One-Line Exam Summary > **Cerebellar lesions produce ipsilateral signs and are managed by treating the cause, controlling complications, and long-term neurorehabilitation.** If you want next: * **30 hard case-based MCQs** * **HTML/CSS/JS interactive exam module** * **Cerebellar syndromes comparison table** * **SEO FAQ schema for cerebellar lesions** Just tell me.
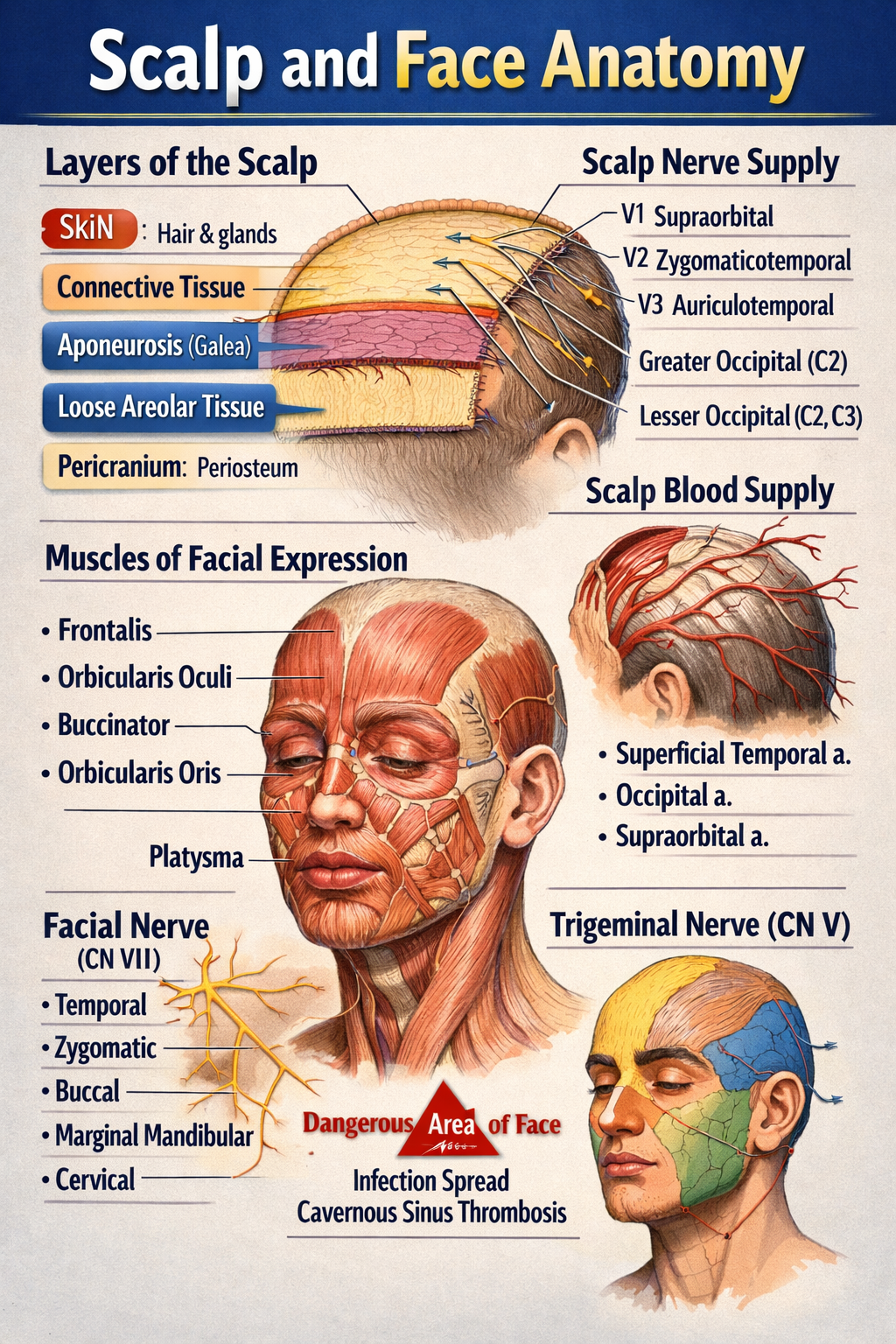
Scalp and Face Anatomy Complete Structure Nerves Blood Supply and Clinical Correlation
Below is a **complete, structured, exam-oriented yet clinically relevant explanation of SCALP AND FACE ANATOMY** — **text only, no images**, written clearly for medical students and healthcare learners. --- # SCALP AND FACE ANATOMY – COMPLETE DETAILED GUIDE --- ## PART A: SCALP ANATOMY ### 1. Definition The **scalp** is the soft tissue covering the cranial vault, extending: * **Anteriorly**: up to the supraorbital margins * **Posteriorly**: to the superior nuchal lines * **Laterally**: to the zygomatic arches --- ### 2. Layers of the Scalp (Mnemonic: **SCALP**) 1. **S – Skin** * Thick, hair-bearing * Rich in sebaceous and sweat glands * Contains hair follicles * Highly vascular → profuse bleeding from cuts 2. **C – Connective Tissue (Dense)** * Fibrofatty layer * Contains **blood vessels and nerves** * Vessels are fixed → cannot retract → excessive bleeding 3. **A – Aponeurosis (Galea Aponeurotica)** * Tough fibrous sheet * Connects: * **Frontalis muscle (anterior)** * **Occipitalis muscle (posterior)** * Lacerations here gape widely 4. **L – Loose Areolar Tissue** * Also called **“danger area of scalp”** * Allows movement of upper 3 layers * Contains emissary veins → connects scalp veins to intracranial venous sinuses * Infection may spread → **cavernous sinus thrombosis / meningitis** 5. **P – Pericranium** * Periosteum covering skull bones * Loosely attached except at sutures * Subperiosteal hematoma limited by sutures --- ### 3. Muscles of the Scalp **Occipitofrontalis muscle** * Frontal belly: elevates eyebrows, wrinkles forehead * Occipital belly: retracts scalp * Innervation: **Facial nerve (CN VII)** --- ### 4. Blood Supply of Scalp #### Arteries (ECA + ICA branches) * **From External Carotid Artery** * Superficial temporal artery * Posterior auricular artery * Occipital artery * **From Internal Carotid Artery (Ophthalmic branch)** * Supraorbital artery * Supratrochlear artery --- ### 5. Venous Drainage * Superficial temporal vein * Posterior auricular vein * Occipital vein → drain into **external jugular vein** **Emissary veins** * Connect extracranial veins to intracranial sinuses * Pathway for infection spread --- ### 6. Nerve Supply of Scalp #### Sensory (Trigeminal + Cervical nerves) * **Anterior to auricle** * Supraorbital nerve (V1) * Supratrochlear nerve (V1) * Zygomaticotemporal nerve (V2) * Auriculotemporal nerve (V3) * **Posterior to auricle** * Greater occipital nerve (C2) * Lesser occipital nerve (C2) * Third occipital nerve (C3) #### Motor * Facial nerve (CN VII) → occipitofrontalis --- ### 7. Applied Anatomy of Scalp * Scalp wounds bleed profusely * Loose areolar tissue → danger area * Cephalhematoma (subperiosteal) * Caput succedaneum (superficial swelling) --- --- ## PART B: FACE ANATOMY --- ### 1. Definition The **face** is the anterior part of the head extending: * From the hairline to the chin * Between the ears laterally --- ### 2. Muscles of Facial Expression * Derived from **second pharyngeal arch** * Insert into skin → facial expressions * Supplied by **Facial nerve (CN VII)** #### Major Groups **Orbital group** * Orbicularis oculi (closes eye) **Oral group** * Orbicularis oris (closes mouth) * Buccinator (cheek muscle) **Nasal group** * Nasalis * Levator labii superioris alaeque nasi --- ### 3. Blood Supply of Face #### Arteries (External Carotid mainly) * Facial artery * Superficial temporal artery * Maxillary artery **Dangerous area of face** * Upper lip, nose, medial cheek * Infection may spread via angular vein → cavernous sinus --- ### 4. Venous Drainage of Face * Facial vein * Angular vein * Retromandibular vein **Communicates with cavernous sinus via** * Ophthalmic veins --- ### 5. Nerve Supply of Face #### Sensory – Trigeminal Nerve (CN V) * **Ophthalmic (V1)**: forehead, upper eyelid * **Maxillary (V2)**: cheek, upper lip * **Mandibular (V3)**: lower lip, chin #### Motor – Facial Nerve (CN VII) Branches within parotid gland: * Temporal * Zygomatic * Buccal * Marginal mandibular * Cervical (Mnemonic: **To Zanzibar By Motor Car**) --- ### 6. Lymphatic Drainage of Face * Submental nodes (chin, lower lip) * Submandibular nodes (cheeks, upper lip) * Preauricular nodes (lateral face) --- ### 7. Skin of Face * Thin, highly vascular * Rich sebaceous glands * Heals well with minimal scarring --- ### 8. Applied Anatomy of Face * Bell’s palsy → facial nerve paralysis * Trigeminal neuralgia * Cavernous sinus thrombosis * Facial nerve injury during parotid surgery * Acne common due to sebaceous glands --- ## QUICK EXAM SUMMARY * **Scalp layers**: Skin, Connective tissue, Aponeurosis, Loose areolar tissue, Pericranium * **Danger areas**: Loose areolar tissue of scalp, Central face * **Motor nerve of face**: Facial nerve (CN VII) * **Sensory nerve of face**: Trigeminal nerve (CN V) * **Main artery of face**: Facial artery --- If you want next: * **MCQs (hard + case based)** * **Clinical correlations only** * **Embryological basis** * **SEO-optimized version** * **Notes in table format** Just tell me 👍
Comments & Discussion
Use this thread like a mini viva: add differentials, staging systems, drug regimens and exam tricks.
Login or register to comment.
No comments yet – start by adding exam-style discussion points.