Clinical videos + HTML notes for NEET PG-ready revision.
Streamora lets you upload case-based videos, attach rich HTML notes, like and comment on other clinicians’ posts, follow creators and save structured exam-oriented pearls – all mobile-first and SEO-ready.
Why Streamora stands out for NEET PG aspirants: Unlike generic apps, we focus on high-yield topics like labour stages (from first to fourth, with management pitfalls), Rh-negative pregnancies (anti-D prophylaxis timing), and anatomy pearls (e.g., sacral hiatus for caudal blocks). Our community-driven notes include real residency cases—e.g., "Missed Rh isoimmunization leading to hydrops fetalis"—with attached flowcharts and MCQ-style tags for quick revision. Free, ad-light, and built by med students for med students.
Latest Medical Posts
High-yield medical discussions, NEET PG-flavoured notes and short clinical cases from all users.
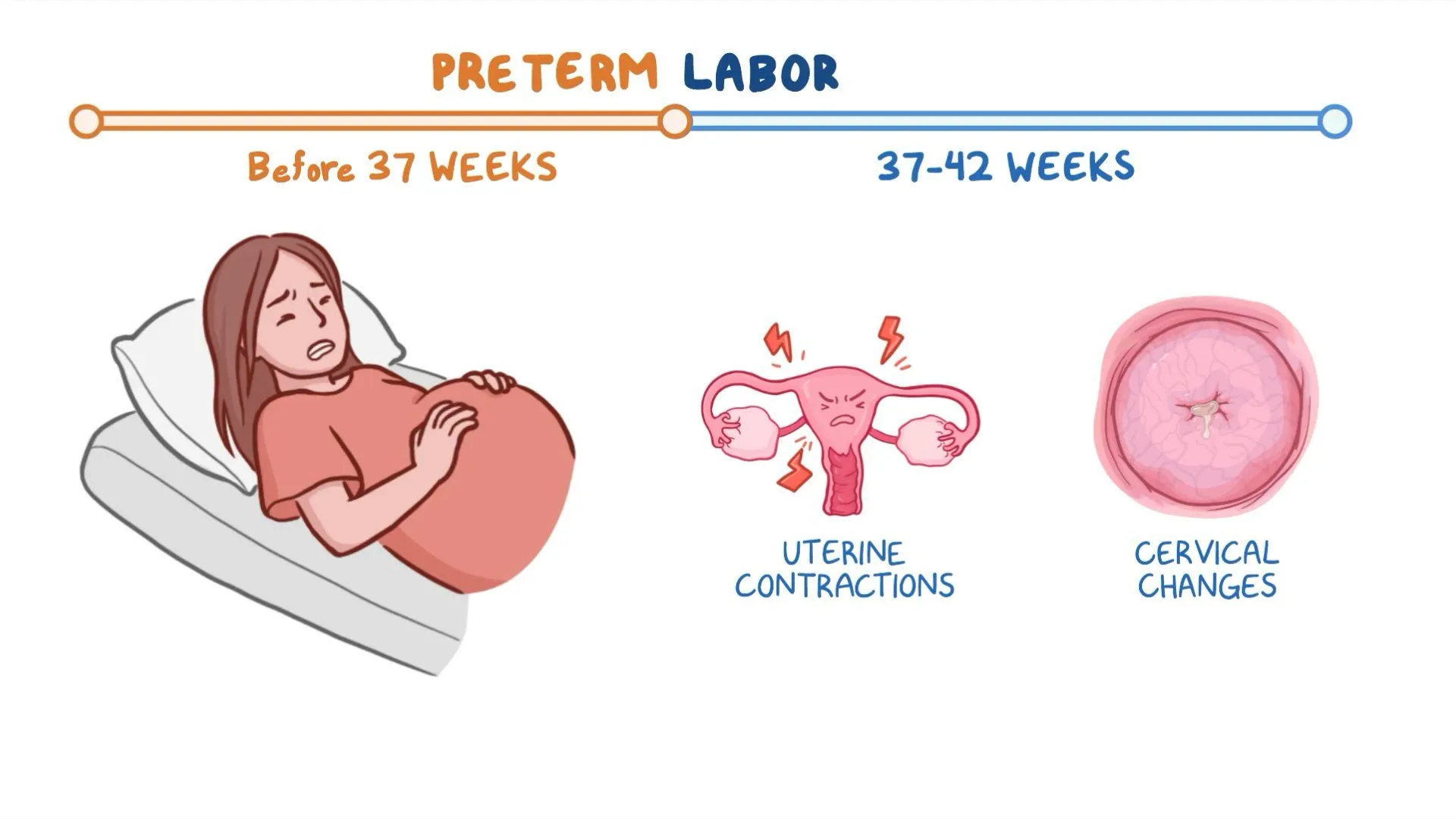
Preterm Labor: Causes, Diagnosis, Prevention and Management
Below is a **single-place, SEO-optimized, exam-ready and clinically complete reference** on **Preterm Labor**, written with clear **H1–H4 structure**, high-value keywords, and authoritative medical depth. --- # **Preterm Labor: Causes, Diagnosis, Prevention and Management** ## **Definition of Preterm Labor** Preterm labor is defined as **regular uterine contractions associated with cervical changes occurring between 20 weeks and before 37 completed weeks of gestation**, leading to preterm birth if not arrested. --- ## **Epidemiology and Importance** * Accounts for **10–12% of all pregnancies globally** * Major cause of **neonatal morbidity and mortality** * Responsible for complications such as **respiratory distress syndrome, intraventricular hemorrhage, necrotizing enterocolitis, sepsis, and long-term neurodevelopmental disability** --- ## **Pathophysiology of Preterm Labor** Preterm labor results from **premature activation of the normal labor pathway**, involving: ### **1. Uterine Activation** * Increased **oxytocin receptors** * Enhanced **prostaglandin synthesis** ### **2. Cervical Ripening** * Collagen degradation * Increased inflammatory mediators ### **3. Decidual and Membrane Activation** * Infection or inflammation leads to cytokine release * Prostaglandins stimulate uterine contractions --- ## **Etiology and Risk Factors** ### **Maternal Factors** * Previous preterm birth * Short interpregnancy interval * Extremes of maternal age * Smoking, substance abuse * Poor antenatal care * Low socioeconomic status ### **Obstetric Factors** * Multiple pregnancy * Polyhydramnios * Placental abruption * Placenta previa * Uterine anomalies ### **Infective Causes** * Urinary tract infection * Bacterial vaginosis * Chorioamnionitis ### **Fetal Factors** * Congenital anomalies * Fetal distress --- ## **Clinical Features of Preterm Labor** ### **Symptoms** * Regular uterine contractions (≥4 in 20 minutes or ≥8 in 60 minutes) * Lower abdominal or back pain * Pelvic pressure * Increased vaginal discharge * Vaginal spotting or bleeding ### **Signs** * Cervical dilation ≥1 cm * Cervical effacement ≥80% * Shortened cervical length on ultrasound --- ## **Diagnosis of Preterm Labor** ### **Clinical Assessment** * History of contractions and risk factors * Sterile speculum examination ### **Investigations** #### **1. Transvaginal Ultrasound** * Cervical length <25 mm before 24 weeks suggests high risk #### **2. Fetal Fibronectin Test** * Positive test indicates increased risk of preterm birth within 7–14 days #### **3. Laboratory Tests** * Urine analysis and culture * High vaginal swab if infection suspected * Complete blood count and CRP when indicated --- ## **Differential Diagnosis** * Braxton Hicks contractions * Urinary tract infection * Abruptio placentae * Placenta previa * Gastrointestinal causes --- ## **Management of Preterm Labor** ### **General Principles** * Confirm diagnosis * Exclude contraindications to tocolysis * Assess gestational age and fetal wellbeing --- ### **Tocolytic Therapy** Used to **delay delivery for 48 hours** to allow steroid administration. #### **1. Nifedipine (First Line)** * **Indication:** Suppression of uterine contractions * **Mechanism:** Calcium channel blockade * **Dose:** 20–30 mg orally loading, then 10–20 mg every 6–8 hours * **Adverse Effects:** Hypotension, headache, flushing * **Contraindications:** Hypotension, cardiac disease * **Monitoring:** Blood pressure, pulse * **Counselling:** Avoid sudden posture changes #### **2. Atosiban** * Oxytocin receptor antagonist * Preferred in cardiac disease #### **3. Indomethacin** * Used before 32 weeks * Risk of premature ductus arteriosus closure --- ### **Antenatal Corticosteroids** Enhance fetal lung maturity. #### **Betamethasone** * **Dose:** 12 mg IM, two doses 24 hours apart * **Benefits:** Reduces RDS, IVH, NEC, neonatal mortality * **Monitoring:** Blood glucose in diabetics --- ### **Magnesium Sulfate for Neuroprotection** * **Indication:** <32 weeks gestation * **Benefit:** Reduces cerebral palsy risk * **Adverse Effects:** Flushing, respiratory depression * **Monitoring:** Reflexes, urine output, respiratory rate --- ### **Antibiotics** * Not routinely indicated * Used when infection is confirmed or suspected --- ## **Contraindications to Tocolysis** * Intrauterine fetal demise * Lethal fetal anomalies * Severe preeclampsia or eclampsia * Chorioamnionitis * Significant vaginal bleeding --- ## **Prevention of Preterm Labor** ### **Primary Prevention** * Smoking cessation * Treatment of genital and urinary infections * Adequate antenatal care ### **Secondary Prevention** #### **Progesterone Therapy** * **Indication:** Previous preterm birth or short cervix * **Dose:** Vaginal progesterone 200 mg daily * **Mechanism:** Maintains uterine quiescence #### **Cervical Cerclage** * Indicated in cervical insufficiency * Performed between 12–14 weeks in selected cases --- ## **Complications** ### **Maternal** * Operative delivery * Infection * Postpartum hemorrhage ### **Neonatal** * Respiratory distress syndrome * Sepsis * Long-term neurodevelopmental impairment --- ## **Prognosis** * Depends on **gestational age at delivery** * Survival improves significantly after **32–34 weeks** * Early recognition and management improve outcomes --- ## **Key Clinical Pearls** * Cervical length is the **best predictor** of preterm birth * Tocolytics delay labor but **do not prevent preterm birth** * Corticosteroids are the **most effective intervention** for neonatal outcomes * Magnesium sulfate provides **neuroprotection**, not tocolysis --- ## **SEO Keywords (Comma Separated)** preterm labor, premature labor, causes of preterm labor, diagnosis of preterm labor, management of preterm labor, tocolytic therapy, antenatal corticosteroids, magnesium sulfate neuroprotection, cervical length ultrasound, fetal fibronectin test, prevention of preterm birth, progesterone therapy pregnancy --- If you want, I can **next provide**: * **25 hard case-based MCQs using HTML CSS JS (single file)** * **FAQs for SEO rich results** * **Schema-ready medical content** * **Exam-oriented summary tables** Just tell me 👍
Twin Pregnancy Complete Guide 2025 Causes Types Diagnosis Risks and Management
Below is a **complete, detailed, SEO-friendly medical article on Twin Pregnancy**, written **without images**, structured with clear **H1–H3 headings**, and optimized for **search engines and medical learning**. --- ## **SEO Title** Twin Pregnancy Complete Guide 2025 Causes Types Diagnosis Risks and Management --- ## **Meta Description** Comprehensive medical guide on twin pregnancy covering types, causes, diagnosis, antenatal care, complications, fetal surveillance, delivery planning, and prognosis for mother and babies. --- ## **SEO Keywords** twin pregnancy, multiple pregnancy twins, dichorionic twins, monochorionic twins, twin pregnancy diagnosis, twin pregnancy complications, twin pregnancy antenatal care, twin pregnancy delivery, twin pregnancy risks, twin pregnancy management, twin gestation obstetrics --- # **Twin Pregnancy** ## **1. Definition** Twin pregnancy is a type of **multiple gestation** in which **two fetuses develop simultaneously in the uterus**. It carries **higher maternal and fetal risks** compared to singleton pregnancy and requires **specialized antenatal monitoring and delivery planning**. --- ## **2. Epidemiology** * Incidence: **1 in 80–90 pregnancies** * Higher incidence with: * Assisted reproductive techniques * Advanced maternal age * Family history of twins * Multiparity --- ## **3. Classification of Twin Pregnancy** ### **3.1 Based on Zygosity** * **Dizygotic (Fraternal) Twins** * Fertilization of two separate ova * Always dichorionic and diamniotic * Most common type * **Monozygotic (Identical) Twins** * Division of a single fertilized ovum * Chorionicity depends on timing of division --- ### **3.2 Based on Chorionicity and Amnionicity** #### **3.2.1 Dichorionic Diamniotic Twins (DCDA)** * Two placentas, two amniotic sacs * Lowest complication rate * May have fused placentas #### **3.2.2 Monochorionic Diamniotic Twins (MCDA)** * One placenta, two amniotic sacs * Risk of twin-to-twin transfusion syndrome #### **3.2.3 Monochorionic Monoamniotic Twins (MCMA)** * One placenta, one amniotic sac * Highest risk * Cord entanglement common --- ## **4. Etiology and Risk Factors** * Assisted reproductive technology * Ovulation induction * Maternal age above 30 years * African ethnicity * Tall stature and high BMI * Family history of twins --- ## **5. Diagnosis of Twin Pregnancy** ### **5.1 Clinical Features** * Excessive uterine enlargement * Severe nausea and vomiting * Early perception of fetal movements * Palpation of multiple fetal parts ### **5.2 Ultrasonography** * Gold standard for diagnosis * Confirms: * Number of fetuses * Chorionicity and amnionicity * Gestational age * Placental location ### **5.3 Doppler Studies** * Used for fetal surveillance * Essential in monochorionic twins --- ## **6. Antenatal Care in Twin Pregnancy** ### **6.1 General Principles** * More frequent antenatal visits * Early booking * Multidisciplinary approach ### **6.2 Nutritional Requirements** * Increased calorie intake * Iron supplementation * Folic acid * Calcium and protein supplementation ### **6.3 Fetal Surveillance** * Serial growth scans every 2–4 weeks * Amniotic fluid assessment * Doppler velocimetry --- ## **7. Maternal Complications** * Anemia * Gestational hypertension * Preeclampsia * Gestational diabetes * Antepartum hemorrhage * Polyhydramnios * Increased operative delivery * Postpartum hemorrhage --- ## **8. Fetal Complications** * Preterm birth * Low birth weight * Intrauterine growth restriction * Congenital anomalies * Twin-to-twin transfusion syndrome * Cord accidents * Perinatal mortality --- ## **9. Special Complications in Monochorionic Twins** ### **9.1 Twin-to-Twin Transfusion Syndrome** * Unequal placental blood flow * Donor twin: growth restriction, oligohydramnios * Recipient twin: polyhydramnios, cardiac overload ### **9.2 Twin Anemia Polycythemia Sequence** * Chronic intertwin blood transfusion * Diagnosed by Doppler MCA PSV --- ## **10. Management of Twin Pregnancy** ### **10.1 Antenatal Management** * Strict blood pressure monitoring * Early detection of complications * Corticosteroids for lung maturity if preterm risk ### **10.2 Timing of Delivery** * DCDA twins: 37–38 weeks * MCDA twins: 36–37 weeks * MCMA twins: 32–34 weeks by planned cesarean ### **10.3 Mode of Delivery** * Vaginal delivery if: * First twin cephalic * No obstetric contraindications * Cesarean section if: * First twin non-cephalic * Monoamniotic twins * Obstetric complications --- ## **11. Intrapartum Care** * Continuous fetal monitoring * Availability of neonatal intensive care * Skilled obstetric and anesthetic support --- ## **12. Postpartum Care** * Active management of third stage * Monitoring for postpartum hemorrhage * Lactation support * Neonatal care for prematurity --- ## **13. Prognosis** * Improved outcomes with early diagnosis * Chorionicity is the strongest predictor * Higher neonatal morbidity compared to singleton pregnancy --- ## **14. Key Clinical Pearls** * Early determination of chorionicity is critical * Monochorionic twins require closer surveillance * Preterm birth is the most common complication * Delivery planning should be individualized --- If you want, I can next provide: **25 hard case-based MCQs (HTML CSS JS single file)**, **FAQs for SEO**, or **exam-oriented short notes** for twin pregnancy.

Placenta Accreta Spectrum: Definition, Risk Factors, Diagnosis and Management
Below is a **fully SEO-optimized, image-free, exam-ready and clinically complete** article on **Placenta Accreta Spectrum**, structured exactly in the **H1 → H2 → H3** format that search engines and medical readers prefer. --- ## **SEO Title** **Placenta Accreta Spectrum: Definition, Risk Factors, Diagnosis and Management** --- ## **SEO Meta Description** Comprehensive clinical guide on Placenta Accreta Spectrum covering definition, types, pathophysiology, risk factors, diagnosis, imaging criteria, antenatal planning, surgical management, complications, and maternal outcomes. --- ## **SEO Keywords** placenta accreta spectrum, placenta accreta, placenta increta, placenta percreta, morbidly adherent placenta, placenta accreta diagnosis, placenta accreta ultrasound signs, placenta accreta MRI, placenta accreta management, cesarean hysterectomy accreta, postpartum hemorrhage accreta --- # **Placenta Accreta Spectrum** ## **1. Definition** Placenta Accreta Spectrum (PAS) refers to a group of abnormal placental attachment disorders characterized by **pathological adherence of the placenta to the myometrium due to partial or complete absence of decidua basalis**, resulting in failure of normal placental separation after delivery. --- ## **2. Classification of Placenta Accreta Spectrum** ### **2.1 Placenta Accreta** * Chorionic villi attach **directly to the myometrium** * Most common and least severe form ### **2.2 Placenta Increta** * Chorionic villi **invade into the myometrium** ### **2.3 Placenta Percreta** * Chorionic villi **penetrate through the myometrium and serosa** * May invade adjacent organs (bladder most commonly) --- ## **3. Epidemiology** * Incidence: ~1 in 300–500 pregnancies * Rapidly increasing due to rising cesarean section rates * Major cause of **severe obstetric hemorrhage and maternal morbidity** --- ## **4. Etiopathogenesis and Pathophysiology** ### **4.1 Underlying Mechanism** * Defective or absent decidua basalis * Inadequate Nitabuch’s layer * Direct trophoblastic invasion into myometrium ### **4.2 Contributing Factors** * Prior uterine surgery leads to **endometrial scarring** * Implantation over scar tissue promotes abnormal placental adherence --- ## **5. Risk Factors** ### **5.1 Major Risk Factors** * Previous cesarean delivery (risk increases with number) * Placenta previa with prior cesarean section ### **5.2 Additional Risk Factors** * Previous myomectomy * Dilatation and curettage * Asherman syndrome * Advanced maternal age * Multiparity * Assisted reproductive techniques --- ## **6. Clinical Features** ### **6.1 Antenatal Period** * Often asymptomatic * Frequently associated with placenta previa * May present with painless antepartum bleeding ### **6.2 Intrapartum and Postpartum** * Failure of placental separation * Massive postpartum hemorrhage * Hypovolemic shock * Disseminated intravascular coagulation --- ## **7. Diagnosis** ### **7.1 Antenatal Diagnosis** Early diagnosis is critical for reducing morbidity. #### **Ultrasound (First Line)** Key grayscale and Doppler findings: * Loss of retroplacental clear zone * Thinning of myometrium (<1 mm) * Placental lacunae (“Swiss cheese” appearance) * Turbulent lacunar blood flow * Bridging vessels to bladder #### **MRI (Adjunct Tool)** Indications: * Posterior placenta * Suspected placenta percreta * Inconclusive ultrasound MRI Findings: * Dark intraplacental bands on T2 * Myometrial thinning * Uterine bulging * Direct invasion of adjacent organs --- ## **8. Differential Diagnosis** * Retained placenta * Uterine atony * Placenta previa without invasion * Uterine inversion --- ## **9. Antenatal Management and Planning** ### **9.1 Multidisciplinary Approach** * Obstetrician * Anesthesiologist * Interventional radiologist * Urologist * Blood bank support ### **9.2 Timing of Delivery** * Planned delivery at **34–36 weeks** * After corticosteroids for fetal lung maturity ### **9.3 Place of Delivery** * Tertiary care center with massive transfusion capability --- ## **10. Intrapartum Management** ### **10.1 Preferred Surgical Approach** * **Planned cesarean hysterectomy without attempting placental removal** * Placenta left in situ to prevent catastrophic hemorrhage ### **10.2 Surgical Principles** * Vertical uterine incision away from placenta * Avoid placental manipulation * Early hysterectomy following fetal delivery --- ## **11. Conservative Management Options** Reserved for highly selected cases desiring fertility. ### **11.1 Methods** * Placenta left in situ * Uterine artery embolization * Methotrexate use (controversial) ### **11.2 Risks** * Severe infection * Delayed hemorrhage * Secondary hysterectomy --- ## **12. Complications** ### **12.1 Maternal Complications** * Massive hemorrhage * Blood transfusion reactions * Bladder or ureteric injury * Sepsis * Thromboembolism * Maternal mortality ### **12.2 Fetal Complications** * Prematurity * Low birth weight * NICU admission --- ## **13. Prognosis** * Prognosis improves significantly with **antenatal diagnosis** * Planned surgery reduces maternal mortality * Future fertility usually lost with definitive surgery --- ## **14. Prevention** * Rational use of cesarean sections * Avoid unnecessary uterine curettage * Early risk stratification in placenta previa cases --- ## **15. Key Exam and Clinical Pearls** * Placenta previa with previous cesarean = **PAS until proven otherwise** * Never attempt manual placental removal if accreta suspected * Cesarean hysterectomy is the gold standard management * MRI complements ultrasound, not a replacement --- If you want, I can next provide: * **Case-based MCQs (HTML CSS JS single file)** * **PAS vs Placenta Previa comparison table** * **FAQ section for SEO** * **Schema-ready JSON-LD medical article** Just tell me 👍

Antepartum Hemorrhage (APH): Causes, Symptoms, Diagnosis, Management & Complications
--- # **Antepartum Hemorrhage (APH): Causes, Symptoms, Diagnosis, Management and Complications** --- ## **What Is Antepartum Hemorrhage?** ### **Definition of Antepartum Hemorrhage** Antepartum hemorrhage (APH) is defined as **bleeding from or into the genital tract occurring after 20 weeks of gestation and before the delivery of the fetus**. ### **Meaning of APH in Pregnancy** APH is a **major obstetric emergency** associated with significant **maternal morbidity, fetal hypoxia, preterm birth, and perinatal mortality**. --- ## **Epidemiology of Antepartum Hemorrhage** ### **Incidence of APH** * Occurs in **3–5% of all pregnancies** * Accounts for a large proportion of **emergency obstetric admissions** ### **Maternal and Perinatal Impact** * Major cause of: * Maternal anemia * Hemorrhagic shock * Stillbirth * Neonatal intensive care admission --- ## **Classification of Antepartum Hemorrhage** ### **Placental Causes of Antepartum Hemorrhage** Placental causes account for **approximately 70% of APH cases**. #### **Placenta Previa** Placenta implanted in the **lower uterine segment**, partially or completely covering the internal cervical os. #### **Placental Abruption (Abruptio Placentae)** Premature separation of a **normally situated placenta** after 20 weeks of gestation. #### **Vasa Previa** Fetal blood vessels traverse the membranes over the cervical os, unprotected by placenta or Wharton’s jelly. --- ### **Non-Placental Causes of Antepartum Hemorrhage** #### **Cervical Causes** * Cervical ectropion * Cervicitis * Cervical polyps * Cervical carcinoma #### **Vaginal Causes** * Trauma * Infection * Varicosities --- ### **Unexplained Antepartum Hemorrhage** * No identifiable cause * Occurs in **10–15%** of cases * Still associated with adverse fetal outcomes --- ## **Risk Factors for Antepartum Hemorrhage** ### **Risk Factors for Placenta Previa** * Previous cesarean section * Previous placenta previa * Multiparity * Advanced maternal age * Smoking ### **Risk Factors for Placental Abruption** * Hypertension and preeclampsia * Abdominal trauma * Smoking and cocaine use * Polyhydramnios * Sudden uterine decompression --- ## **Pathophysiology of Antepartum Hemorrhage** ### **Pathophysiology of Placenta Previa** * Placenta in lower uterine segment * Stretching and thinning cause **placental separation** * Results in **painless bleeding** ### **Pathophysiology of Placental Abruption** * Rupture of maternal vessels in decidua basalis * Formation of retroplacental hematoma * Leads to **uterine hypertonicity and fetal hypoxia** ### **Pathophysiology of Vasa Previa** * Rupture of fetal vessels * Rapid fetal blood loss * Can cause **acute fetal demise** --- ## **Clinical Features of Antepartum Hemorrhage** ### **General Symptoms of APH** * Vaginal bleeding * Reduced fetal movements * Abdominal pain (may or may not be present) --- ### **Clinical Features of Placenta Previa** * **Painless**, bright red bleeding * Recurrent episodes * Soft, non-tender uterus * Malpresentation common * Fetal heart sounds usually normal --- ### **Clinical Features of Placental Abruption** * **Painful bleeding** * Dark blood * Tense, tender uterus * Maternal shock may be disproportionate * Fetal distress or absent heart sounds --- ### **Clinical Features of Vasa Previa** * Sudden bleeding after rupture of membranes * Fetal bradycardia * Maternal condition relatively stable --- ## **Initial Assessment of Antepartum Hemorrhage** ### **Primary Survey (ABC Approach)** * Airway, Breathing, Circulation * Oxygen supplementation * Two large-bore IV cannulae * Monitor vitals and urine output ### **Important Clinical Rule** ⚠️ **Digital vaginal examination is contraindicated until placenta previa is excluded** --- ## **Investigations in Antepartum Hemorrhage** ### **Laboratory Investigations** * Complete blood count * Blood group and Rh typing * Cross-match blood * Coagulation profile (especially in abruption) * Renal function tests --- ### **Imaging in Antepartum Hemorrhage** * **Ultrasound** for placental localization * Doppler ultrasound for suspected vasa previa * Continuous CTG for fetal monitoring --- ## **Differential Diagnosis of Antepartum Hemorrhage** * Placenta previa * Placental abruption * Vasa previa * Preterm labor with show * Cervical malignancy * Uterine rupture (rare) --- ## **Management of Antepartum Hemorrhage** ### **General Management Principles** * Hospital admission * Bed rest * IV fluids * Blood transfusion if required * Anti-D immunoglobulin for Rh-negative mothers * Corticosteroids if gestation <34 weeks --- ## **Management of Placenta Previa** ### **Expectant Management** Indicated when: * Bleeding is mild * Gestation is preterm * Mother and fetus stable Includes: * Close monitoring * Avoid vaginal exams * Steroids for fetal lung maturity --- ### **Definitive Management** * **Cesarean section** is the mode of delivery for: * Major placenta previa * Heavy or recurrent bleeding * Fetal distress * Term pregnancy --- ## **Management of Placental Abruption** ### **Mild Abruption** * Conservative management * Close maternal and fetal monitoring ### **Severe Abruption** * Immediate delivery * Blood products * Correction of coagulopathy ### **Mode of Delivery** * Vaginal if fetus dead and labor progressing * Cesarean if fetus alive with distress --- ## **Management of Vasa Previa** * Emergency cesarean section * Neonatal resuscitation readiness * Planned elective cesarean if diagnosed antenatally --- ## **Complications of Antepartum Hemorrhage** ### **Maternal Complications** * Hemorrhagic shock * Disseminated intravascular coagulation (DIC) * Postpartum hemorrhage * Acute kidney injury * Maternal death --- ### **Fetal Complications** * Prematurity * Intrauterine growth restriction * Fetal hypoxia * Stillbirth * Neonatal anemia --- ## **Prevention of Antepartum Hemorrhage** ### **Preventive Strategies** * Routine antenatal ultrasound * Control of hypertension * Avoid smoking and substance abuse * Planned delivery in high-risk pregnancies --- ## **Prognosis of Antepartum Hemorrhage** ### **Maternal Prognosis** * Good with early diagnosis and prompt management ### **Fetal Prognosis** * Depends on: * Cause of APH * Gestational age * Speed of intervention --- ## **Exam-Oriented Key Points** * **Painless bleeding → Placenta previa** * **Painful bleeding + tender uterus → Abruption** * **Shock out of proportion → Concealed abruption** * **Never perform PV exam before ruling out placenta previa** --- ## **Frequently Asked Questions (SEO Boost)** ### **Is antepartum hemorrhage dangerous?** Yes. APH is a **medical emergency** that can threaten both maternal and fetal life. ### **What is the most common cause of APH?** **Placenta previa** is the most common cause. ### **Can APH be prevented?** Some causes can be reduced with proper antenatal care and risk factor control. ---
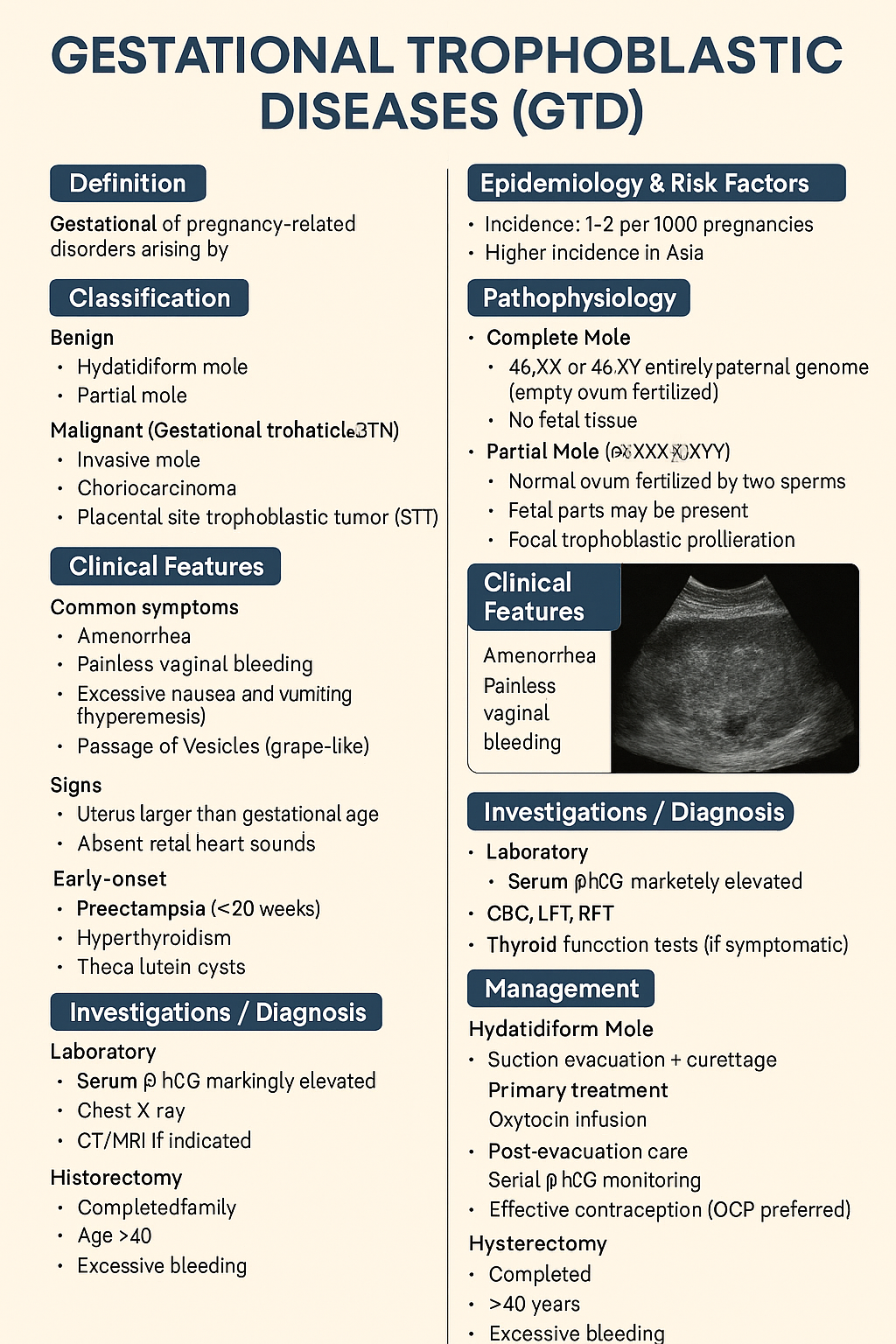
Gestational Trophoblastic Diseases (GTD): Types, Diagnosis, Management & Prognosis – Complete Medical Guide 2025
Below is a **single-place, exam-ready, clinically complete reference** on **Gestational Trophoblastic Diseases (GTD)**, structured exactly for **medical learning, exams, and clinical use**. --- # **Gestational Trophoblastic Diseases (GTD)** ## **1. Definition** Gestational trophoblastic diseases are a **spectrum of pregnancy-related disorders** arising from **abnormal proliferation of trophoblastic tissue** following conception. They range from **benign molar pregnancy** to **malignant gestational trophoblastic neoplasia (GTN)**. --- ## **2. Classification** ### **A. Benign** 1. **Hydatidiform mole** * Complete mole * Partial mole ### **B. Malignant (Gestational Trophoblastic Neoplasia – GTN)** 1. **Invasive mole** 2. **Choriocarcinoma** 3. **Placental site trophoblastic tumor (PSTT)** 4. **Epithelioid trophoblastic tumor (ETT)** --- ## **3. Epidemiology & Risk Factors** * Incidence: **1–2 per 1000 pregnancies** * Higher incidence in **Asia** * Risk factors: * Extremes of maternal age (<20, >35 years) * Previous molar pregnancy * Nutritional deficiency (low carotene, folate) * History of miscarriage --- ## **4. Pathophysiology** ### **Complete Mole** * **46,XX or 46,XY** * Entirely paternal genome (empty ovum fertilized) * No fetal tissue * Diffuse trophoblastic hyperplasia ### **Partial Mole** * **Triploid (69,XXX/XXY/XYY)** * Normal ovum fertilized by two sperms * Fetal parts may be present * Focal trophoblastic proliferation --- ## **5. Clinical Features** ### **Common Symptoms** * Amenorrhea * **Painless vaginal bleeding** * Excessive nausea and vomiting (hyperemesis) * Passage of vesicles (grape-like) ### **Signs** * Uterus larger than gestational age (complete mole) * Absent fetal heart sounds * Early-onset: * Preeclampsia (<20 weeks) * Hyperthyroidism * Theca lutein cysts --- ## **6. Investigations / Diagnosis** ### **Laboratory** * **Serum β-hCG**: markedly elevated * CBC, LFT, RFT * Thyroid function tests (if symptomatic) ### **Imaging** * **Ultrasound** * Complete mole: *“Snowstorm / cluster of grapes”* * Partial mole: gestational sac + abnormal fetus ### **Histopathology** * Confirms diagnosis after evacuation ### **Baseline Metastatic Work-up (GTN)** * Chest X-ray * CT/MRI if indicated --- ## **7. Differential Diagnosis** * Missed abortion * Ectopic pregnancy * Placenta accreta * Degenerating fibroid --- ## **8. Management** ### **A. Hydatidiform Mole** #### **Primary Treatment** * **Suction evacuation + curettage** (treatment of choice) * Oxytocin infusion after evacuation #### **Post-Evacuation Care** * Serial β-hCG monitoring * Effective contraception (OCP preferred) #### **Hysterectomy** * Completed family * Age >40 years * Excessive bleeding --- ### **B. Gestational Trophoblastic Neoplasia (GTN)** #### **Diagnosis of GTN (FIGO criteria)** * Plateauing β-hCG * Rising β-hCG * Persistent β-hCG >6 months * Histologic choriocarcinoma #### **Risk Stratification (WHO Score)** * Low risk: ≤6 * High risk: ≥7 --- ## **9. Chemotherapy** ### **Low-Risk GTN** #### **Methotrexate** * **Mechanism**: Folate antagonist → inhibits DNA synthesis * **Dose**: * 50 mg IM weekly OR * 1 mg/kg on days 1,3,5,7 + folinic acid * **Adverse effects**: * Stomatitis * Hepatotoxicity * Bone marrow suppression * **Monitoring**: * CBC * LFTs * β-hCG weekly * **Contraindications**: * Liver disease * Renal failure #### **Actinomycin-D (Alternative)** * **Mechanism**: DNA intercalation * **Dose**: 1.25 mg/m² IV every 2 weeks * **Adverse effects**: * Alopecia * Myelosuppression --- ### **High-Risk GTN** #### **EMA-CO Regimen** * **Etoposide** * **Methotrexate** * **Actinomycin-D** * **Cyclophosphamide** * **Vincristine** **Indication**: WHO score ≥7 or metastatic disease --- ## **10. Special Types** ### **Choriocarcinoma** * Highly malignant * Early hematogenous spread (lungs, brain) * Very high β-hCG * Responds excellently to chemotherapy ### **PSTT & ETT** * Low β-hCG * Less chemosensitive * **Primary treatment: hysterectomy** --- ## **11. Follow-Up** * β-hCG: * Weekly until negative ×3 * Monthly for 6–12 months * Contraception mandatory during follow-up * Next pregnancy allowed after surveillance completion --- ## **12. Prognosis** * Cure rate: * **>98% in low-risk GTN** * **>85–90% in high-risk GTN** * Future fertility usually preserved --- ## **13. Key Exam Pearls** * Early preeclampsia → think **molar pregnancy** * β-hCG is the **tumor marker** * Choriocarcinoma follows **any pregnancy** * PSTT → **hysterectomy**, not chemo * OCPs are **safe** during follow-up --- If you want next: * **SEO title + keywords** * **25 hard case-based MCQs (HTML/CSS/JS – single file)** * **Flowcharts / tables only** * **Separate GTN chemotherapy comparison** * **Image-free exam revision notes** Just tell me what you want next.
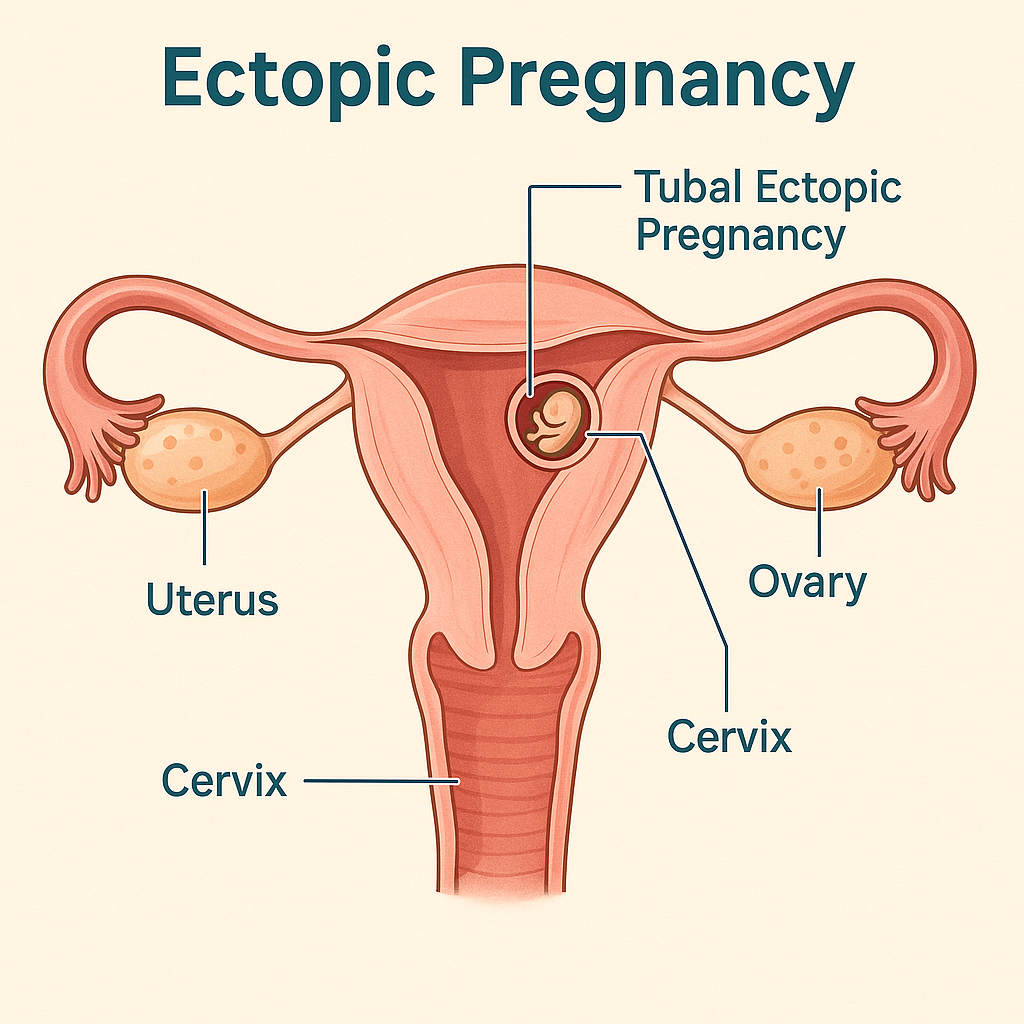
Ectopic Pregnancy: Causes, Symptoms, Diagnosis, Treatment Options & Management Guidelines (2025 Complete Guide)
Below is a **single-place, exam-ready + clinical-practice detailed reference** on **Ectopic Pregnancy**, written in the **structured pattern you prefer** and suitable for your medical hub. ✔️ **No images included** ✔️ **Includes authoritative external links** --- # **Ectopic Pregnancy – Complete Clinical & Management Guide (2025)** --- ## **1. Definition** **Ectopic pregnancy** is implantation of a fertilized ovum **outside the endometrial cavity**. > > 95% occur in the **fallopian tube**. It is a **life-threatening obstetric emergency** if ruptured. --- ## **2. Epidemiology** * Incidence: **1–2% of all pregnancies** * Leading cause of **maternal mortality in first trimester** * Rising incidence due to: * Assisted reproductive techniques (ART) * Pelvic inflammatory disease (PID) --- ## **3. Common Sites of Ectopic Pregnancy** | Site | Approx. % | | ---------------------- | ---------- | | Ampullary tube | 70% | | Isthmic tube | 12% | | Fimbrial | 11% | | Interstitial (cornual) | 2–4% | | Ovarian | <1% | | Cervical | <1% | | Caesarean scar | Increasing | --- ## **4. Pathophysiology** Normal embryo transport is impaired due to: * **Tubal damage** * **Altered tubal motility** * **Delayed ovum transport** → Implantation occurs before reaching uterus → Trophoblastic invasion erodes vessels → **Tubal rupture → hemorrhage** --- ## **5. Risk Factors** ### High-risk * Previous ectopic pregnancy * Tubal surgery / sterilization * PID (especially *Chlamydia*) * Assisted reproduction (IVF) ### Moderate risk * IUCD in situ * Smoking * Endometriosis ### No identifiable risk factor in ~50% --- ## **6. Clinical Features** ### Classical Triad (only ~50%) 1. **Amenorrhea** 2. **Lower abdominal pain** 3. **Vaginal bleeding** ### Other symptoms * Shoulder tip pain (diaphragmatic irritation) * Syncope * Dizziness ### Signs of Rupture * Hypotension * Tachycardia * Pallor * Abdominal guarding * Cervical motion tenderness * Full, tender pouch of Douglas --- ## **7. Investigations / Diagnosis** ### 1. Urine Pregnancy Test * Positive ### 2. Serum β-hCG (Quantitative) * **Discriminatory zone**: ~1500–2000 IU/L * If no intrauterine gestational sac → suspect ectopic * Plateauing or suboptimal rise (<66% in 48 hrs) ### 3. Transvaginal Ultrasound (TVS) **Suggestive findings** * Empty uterus * Adnexal mass * Tubal ring sign * Free fluid in pelvis ### 4. Culdocentesis (obsolete) ### 5. Diagnostic Laparoscopy (gold standard if uncertain) --- ## **8. Differential Diagnosis** * Threatened / incomplete abortion * Corpus luteum cyst * Acute PID * Ovarian torsion * Appendicitis * Renal colic --- ## **9. Management (Stepwise)** ### A. Expectant Management **Criteria** * Asymptomatic * β-hCG <200 IU/L and declining * No adnexal mass * Reliable follow-up --- ### B. Medical Management – **Methotrexate** #### Indications * Hemodynamically stable * Unruptured ectopic * β-hCG ≤5000 IU/L * No fetal cardiac activity #### Contraindications * Hemodynamic instability * Liver, renal disease * Breastfeeding * Blood dyscrasias #### Regimens **Single-dose** * Methotrexate **50 mg/m² IM** * Check β-hCG on day 4 & 7 **Multi-dose** * MTX 1 mg/kg on days 1,3,5,7 * Leucovorin rescue --- ### C. Surgical Management #### Indications * Ruptured ectopic * Hemodynamic instability * Failed medical treatment * Contraindications to methotrexate #### Procedures * **Salpingectomy** (preferred if tube severely damaged) * **Salpingostomy** (fertility preservation) * Laparoscopy preferred over laparotomy (if stable) --- ## **10. Special Types** ### Interstitial (Cornual) * Late rupture * Massive hemorrhage * Managed surgically ± MTX ### Cervical Ectopic * Painless bleeding * Managed with MTX, uterine artery embolization ### Caesarean Scar Pregnancy * Increasing incidence * High risk of placenta accreta * Early MTX or surgical excision --- ## **11. Complications** * Hemorrhagic shock * Infertility * Recurrent ectopic pregnancy * Maternal death (if delayed) --- ## **12. Prognosis** * Future fertility preserved in many * Recurrence risk: **10–25%** * Early diagnosis improves outcomes --- ## **13. Counselling & Follow-Up** * Avoid pregnancy for **3 months after MTX** * Early ultrasound in next pregnancy * Discuss recurrence risk * Rh-negative women → **Anti-D immunoglobulin** --- ## **14. Prevention** * Prompt treatment of PID * Smoking cessation * Safe reproductive practices * Early antenatal booking --- ## **15. Authoritative External Links** * **WHO – Ectopic Pregnancy Overview** [https://www.who.int](https://www.who.int) * **ACOG Practice Bulletin: Tubal Ectopic Pregnancy** [https://www.acog.org](https://www.acog.org) * **RCOG Green-top Guideline No. 21** [https://www.rcog.org.uk](https://www.rcog.org.uk) * **UpToDate – Ectopic Pregnancy (Clinician Reference)** [https://www.uptodate.com](https://www.uptodate.com) * **NICE Guideline: Ectopic pregnancy and miscarriage** [https://www.nice.org.uk](https://www.nice.org.uk) --- If you want, I can next: * Create **SEO title, meta description & keywords** * Convert this into **HTML (single-file)** for your site * Generate **case-based MCQs** * Add **internal links** to abortion, PID, β-hCG interpretation, or early pregnancy bleeding Just tell me 👍
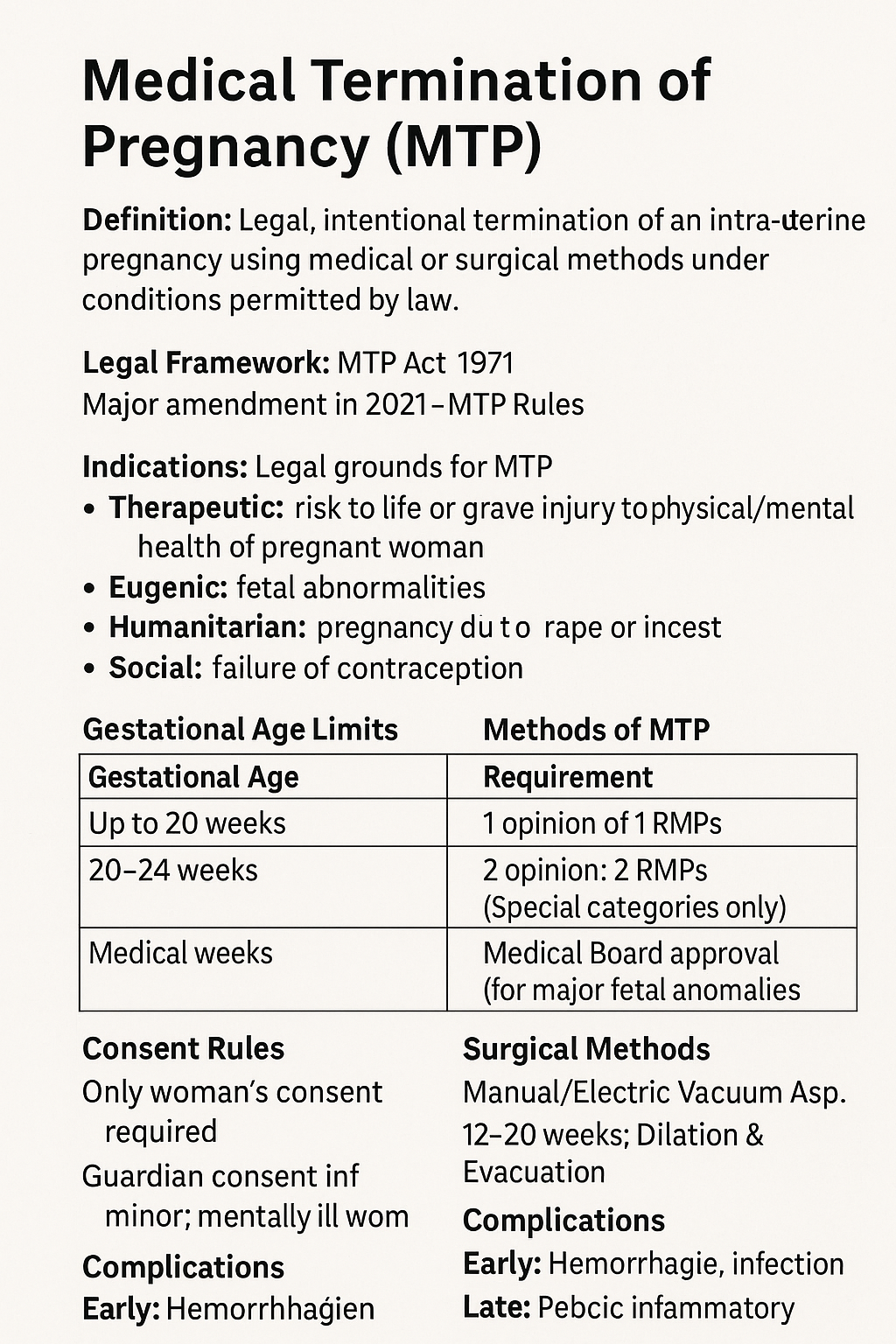
Medical Termination of Pregnancy (MTP): MTP Act, Indications, Methods, Gestational Limits & Complete Guide 2025
Below is a **complete, exam-ready, clinically exhaustive detail note on MTP (Medical Termination of Pregnancy)** with **reliable external reference links**. *(Text only, no images — as you prefer.)* --- # **Medical Termination of Pregnancy (MTP): Complete Detailed Note (India-Focused, 2025)** --- ## **1. Definition** **Medical Termination of Pregnancy (MTP)** is the **legal, intentional termination of an intra-uterine pregnancy** using **medical or surgical methods**, performed **under conditions permitted by law** to safeguard the woman’s physical, mental, and social well-being. --- ## **2. Legal Framework in India** ### **MTP Act** * **MTP Act, 1971** * **Amended in 2002** * **Major Amendment in 2021** * **MTP Rules & Regulations, 2003 & 2021** ### **Key Objectives** * Reduce **unsafe abortions** * Protect **reproductive rights** * Reduce **maternal mortality** --- ## **3. Indications for MTP (Legal Grounds)** ### **A. Therapeutic** * Risk to **life of the pregnant woman** * Grave injury to **physical or mental health** ### **B. Eugenic** * Substantial risk of **serious fetal abnormalities** * Includes **lethal anomalies, chromosomal disorders** ### **C. Humanitarian** * Pregnancy due to **rape or incest** ### **D. Social** * **Failure of contraception** (Applicable to **married & unmarried women** after 2021 amendment) --- ## **4. Gestational Age Limits & Medical Opinion** | Gestational Age | Requirement | | --------------- | ------------------------------------------------------ | | **≤ 20 weeks** | Opinion of **1 Registered Medical Practitioner (RMP)** | | **20–24 weeks** | Opinion of **2 RMPs** (Special categories only) | | **> 24 weeks** | **Medical Board approval** (for major fetal anomalies) | ### **Special Categories (20–24 weeks)** * Survivors of rape/incest * Minors * Differently-abled women * Mentally ill women * Disaster/emergency situations --- ## **5. Who Can Perform MTP?** Only a **Registered Medical Practitioner (RMP)** with: * Recognized qualification * Training in **obstetrics & gynecology** * Performed at **approved facilities only** --- ## **6. Approved Places for MTP** * Government hospitals * Approved private hospitals/clinics * Facilities meeting **MTP Rules infrastructure criteria** --- ## **7. Methods of MTP** --- ### **A. Medical Abortion** **Used up to 9 weeks (63 days)** #### **Drugs & Regimen** 1. **Mifepristone 200 mg orally** 2. After 24–48 hrs → **Misoprostol 800 mcg** * Oral / Buccal / Vaginal #### **Mechanism** * Mifepristone: Progesterone antagonist → decidual breakdown * Misoprostol: Prostaglandin → uterine contractions #### **Contraindications** * Ectopic pregnancy * Chronic adrenal failure * Long-term steroid therapy * Bleeding disorders --- ### **B. Surgical Methods** #### **Up to 12 weeks** * **Manual Vacuum Aspiration (MVA)** * **Electric Vacuum Aspiration (EVA)** #### **12–20 weeks** * **Dilation & Evacuation (D&E)** #### **>20 weeks (selected cases)** * Medical induction using **misoprostol ± mifepristone** * Rarely hysterotomy --- ## **8. Pre-Procedure Evaluation** * Confirm **intrauterine pregnancy** * Gestational age (USG) * Hb, blood group & Rh * Rule out **ectopic pregnancy** * Informed **written consent** * **Guardian consent** for minors/mentally ill women --- ## **9. Consent Rules** * **Only woman’s consent required** * **Husband’s consent NOT required** * Guardian consent mandatory for: * Minor (<18 years) * Mentally ill woman --- ## **10. Confidentiality** * Identity of woman **must not be disclosed** * Breach punishable under law --- ## **11. Post-Abortion Care** * Monitor bleeding, infection * **Anti-D immunoglobulin** for Rh-negative women * Pain management * Antibiotics if indicated * **Contraceptive counselling before discharge** --- ## **12. Complications of MTP** ### **Early** * Hemorrhage * Infection * Incomplete abortion * Uterine perforation (surgical) ### **Late** * Pelvic inflammatory disease * Asherman syndrome (rare) * Psychological distress --- ## **13. Failure of MTP** * Ongoing pregnancy * Incomplete evacuation * Requires repeat evacuation or surgery --- ## **14. MTP vs Illegal Abortion** | Legal MTP | Unsafe Abortion | | -------------- | ----------------------- | | Done by RMP | Untrained person | | Approved place | Unsafe location | | Sterile | Septic | | Low mortality | High maternal mortality | --- ## **15. Ethical & Social Aspects** * Women’s **reproductive autonomy** * Balancing fetal rights & maternal health * Public health importance --- ## **16. Important Exam & Clinical Pearls** * MTP **≠ abortion on demand** * 2021 Act includes **unmarried women** * Husband consent **not required** * Medical Board mandatory **>24 weeks** --- ## **17. Reliable External Reference Links** * **Ministry of Health & Family Welfare (India)** [https://www.mohfw.gov.in](https://www.mohfw.gov.in) * **MTP Act 1971 (Bare Act)** [https://legislative.gov.in/actsofparliamentfromtheyear/medical-termination-pregnancy-act-1971](https://legislative.gov.in/actsofparliamentfromtheyear/medical-termination-pregnancy-act-1971) * **MTP Amendment Act 2021** [https://prsindia.org/billtrack/medical-termination-of-pregnancy-amendment-bill-2020](https://prsindia.org/billtrack/medical-termination-of-pregnancy-amendment-bill-2020) * **WHO – Abortion Care Guideline** [https://www.who.int/publications/i/item/9789240039483](https://www.who.int/publications/i/item/9789240039483) * **ACOG – Induced Abortion** [https://www.acog.org/clinical/clinical-guidance/practice-bulletin](https://www.acog.org/clinical/clinical-guidance/practice-bulletin) * **FIGO Safe Abortion Guidelines** [https://www.figo.org/resources/safe-abortion](https://www.figo.org/resources/safe-abortion) --- If you want, I can next: * Add **SEO title + meta description + keywords** * Convert this into **HTML medical hub format** * Create **case-based MCQs** * Add **Indian court case highlights (landmark judgments)**
Is Pneumonia Contagious? Causes, Transmission, Types, Risk Factors & Prevention Explained
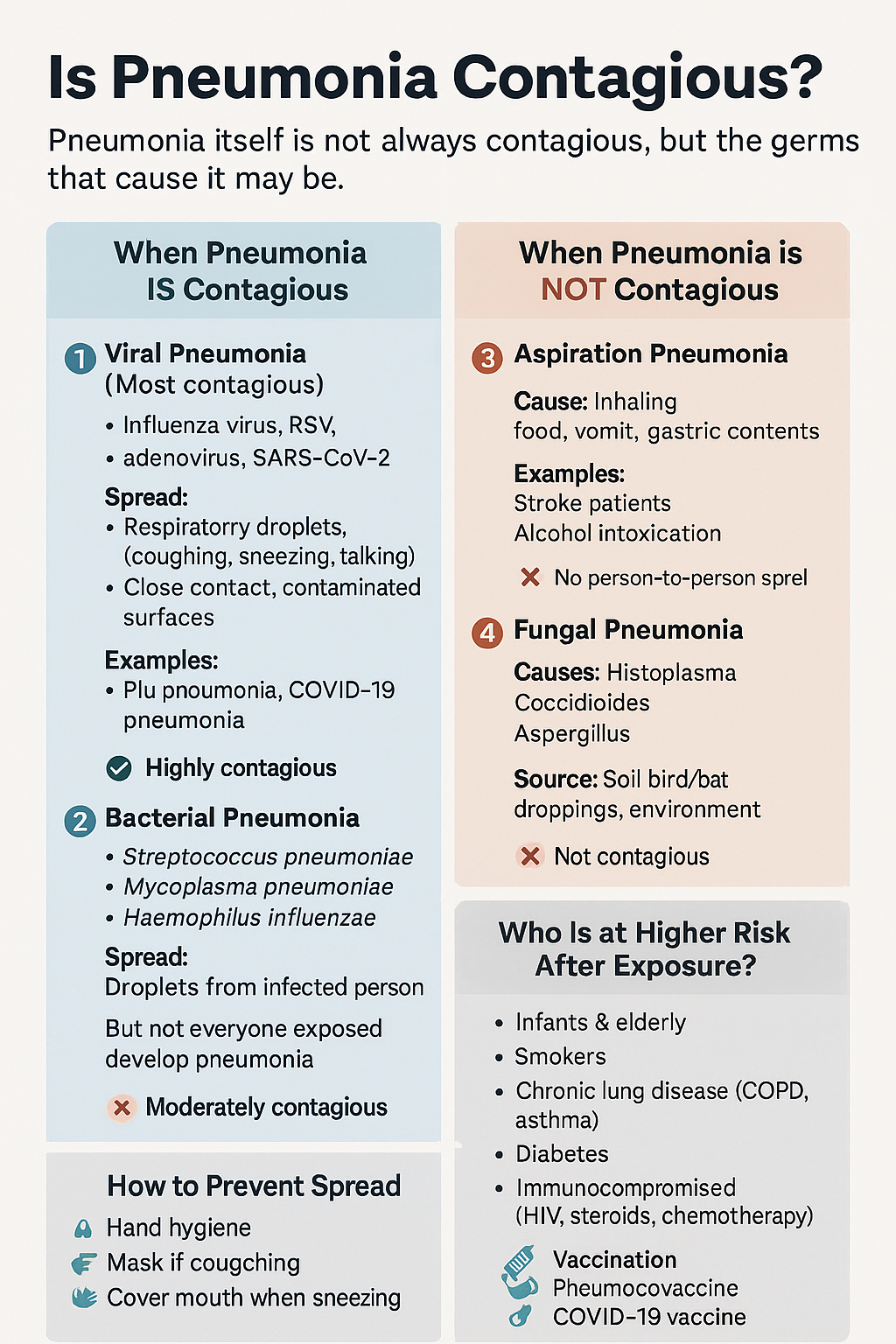
Below is a **detailed, SEO-ready explanation of pneumonia contagion**, written so you can **directly use it on your medical website** and **add internal links to related posts/pages** (topics commonly present in your medical hub). --- # Is Pneumonia Contagious? Causes, Spread, Risk Factors & Prevention (Complete Guide) ## 🔍 Overview **Pneumonia is an infection of the lung parenchyma** causing inflammation of alveoli with fluid or pus accumulation. Whether pneumonia is **contagious or not depends entirely on its cause**, not on the condition itself. 👉 *(Internal link idea: **What is Pneumonia? – Definition, Types & Pathophysiology**)* --- ## 🦠 Is Pneumonia Contagious? ### **Short answer:** ✔️ **Sometimes yes** ❌ **Sometimes no** The **microorganism causing pneumonia may spread**, but **pneumonia as a disease does not directly transmit**. --- ## 1️⃣ Viral Pneumonia (Highly Contagious) **Most common contagious form** ### Common Causes * Influenza virus * Respiratory Syncytial Virus (RSV) * Adenovirus * SARS-CoV-2 (COVID-19) 👉 *(Internal link: **Viral Pneumonia – Causes, Symptoms & Treatment**)* ### Mode of Spread * Respiratory droplets (coughing, sneezing, talking) * Close personal contact * Contaminated surfaces ### Contagious Period * **1–2 days before symptoms** * **5–7 days after symptom onset** * Longer in children and immunocompromised patients ### Key Point > Viral pneumonia spreads easily, especially in **crowded places, households, and hospitals**. --- ## 2️⃣ Bacterial Pneumonia (Moderately Contagious) ### Common Causes * *Streptococcus pneumoniae* * *Haemophilus influenzae* * *Mycoplasma pneumoniae* * *Chlamydia pneumoniae* 👉 *(Internal link: **Bacterial Pneumonia – Diagnosis & Antibiotic Management**)* ### Spread * Respiratory droplets * Close contact with infected person ⚠️ **Important:** You may catch the bacteria, but **only susceptible individuals develop pneumonia**. ### After Treatment * **Not contagious after 24–48 hours of effective antibiotics** --- ## 3️⃣ Aspiration Pneumonia (Not Contagious) ### Cause * Inhalation of: * Food particles * Vomit * Gastric acid * Oropharyngeal secretions 👉 *(Internal link: **Aspiration Pneumonia – Risk Factors & Prevention**)* ### Common in * Stroke patients * Alcohol intoxication * Elderly with swallowing disorders * ICU patients ❌ **No person-to-person spread** --- ## 4️⃣ Fungal Pneumonia (Not Contagious) ### Causes * *Histoplasma* * *Coccidioides* * *Aspergillus* 👉 *(Internal link: **Fungal Lung Infections – Clinical Features & Treatment**)* ### Transmission * Inhalation of spores from: * Soil * Bird or bat droppings * ❌ **No human-to-human transmission** --- ## 👥 Who Is More Likely to Get Pneumonia After Exposure? * Infants & elderly * Smokers * COPD or asthma patients * Diabetes mellitus * Immunocompromised (HIV, chemotherapy, steroids) 👉 *(Internal link: **Risk Factors for Severe Pneumonia**)* --- ## 🛡️ How to Prevent Spread of Contagious Pneumonia * Hand hygiene 🧼 * Mask use during respiratory illness 😷 * Cover mouth while coughing/sneezing * Avoid close contact during active infection * Vaccination: * **Influenza vaccine** * **Pneumococcal vaccine** * **COVID-19 vaccine** 👉 *(Internal link: **Vaccines That Prevent Pneumonia**)* --- ## 🧠 Key Takeaway > **Pneumonia is contagious only when caused by infectious agents like viruses or bacteria.** > Aspiration and fungal pneumonias **do not spread from person to person**. --- ## 🔗 Suggested Internal Linking Structure (SEO Boost) Use internal links to: * Pneumonia Types * Viral vs Bacterial Pneumonia * Pneumonia Symptoms * Pneumonia Diagnosis * Pneumonia Treatment Guidelines * Pneumonia Complications * Pneumonia Prevention & Vaccination This improves **topical authority**, **crawl depth**, and **search ranking**. --- If you want, I can next: * Add **HTML internal link anchors** for your site * Create **schema-ready medical content** * Generate **SEO title, meta description & keywords** * Convert this into **exam-oriented notes or patient-friendly version** Just tell me what you want next 👍
Is Pneumonia Contagious? Causes, Transmission, Types, Risk Factors & Prevention Explained
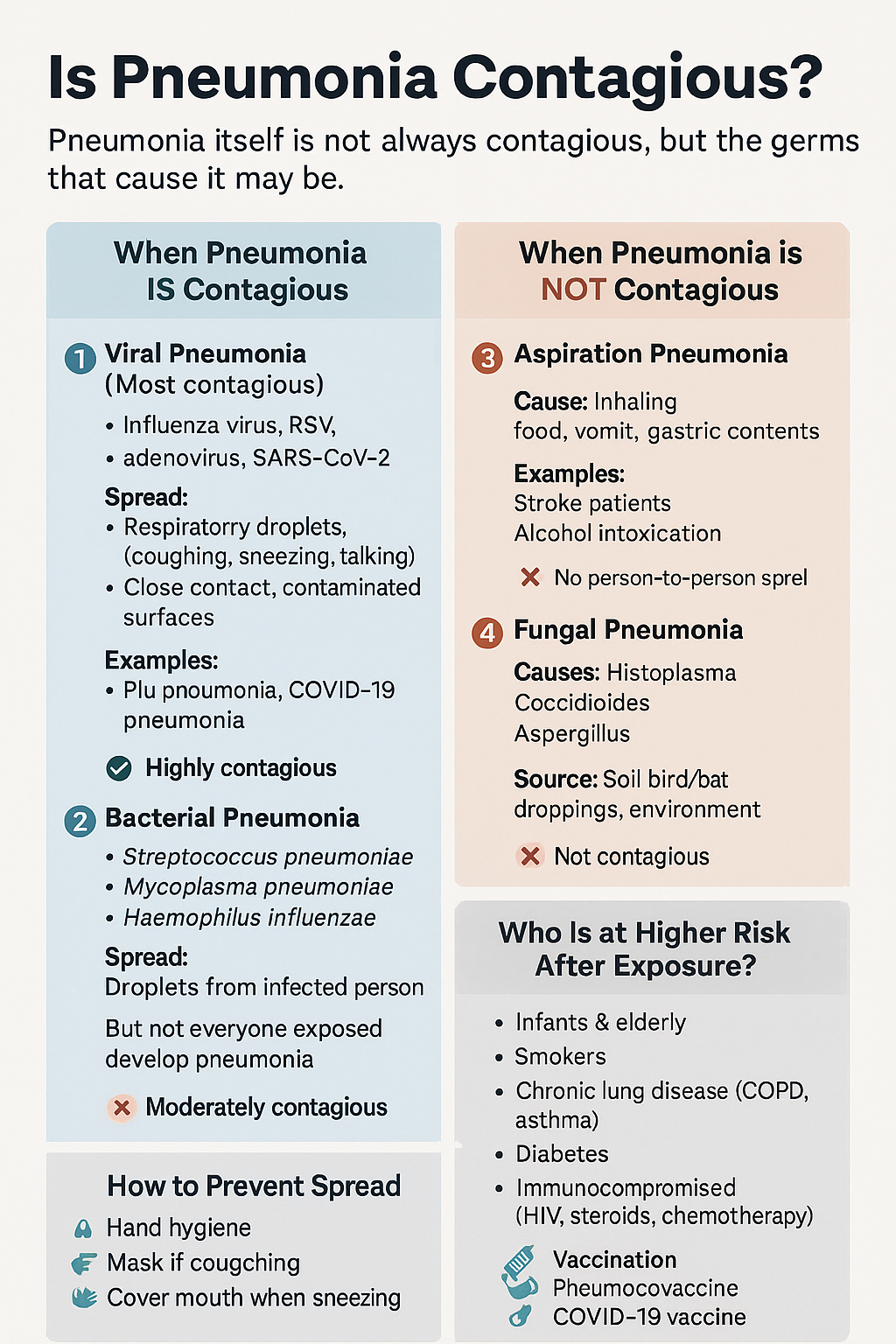
Below is a **detailed, SEO-ready explanation of pneumonia contagion**, written so you can **directly use it on your medical website** and **add internal links to related posts/pages** (topics commonly present in your medical hub). --- # Is Pneumonia Contagious? Causes, Spread, Risk Factors & Prevention (Complete Guide) ## 🔍 Overview **Pneumonia is an infection of the lung parenchyma** causing inflammation of alveoli with fluid or pus accumulation. Whether pneumonia is **contagious or not depends entirely on its cause**, not on the condition itself. 👉 *(Internal link idea: **What is Pneumonia? – Definition, Types & Pathophysiology**)* --- ## 🦠 Is Pneumonia Contagious? ### **Short answer:** ✔️ **Sometimes yes** ❌ **Sometimes no** The **microorganism causing pneumonia may spread**, but **pneumonia as a disease does not directly transmit**. --- ## 1️⃣ Viral Pneumonia (Highly Contagious) **Most common contagious form** ### Common Causes * Influenza virus * Respiratory Syncytial Virus (RSV) * Adenovirus * SARS-CoV-2 (COVID-19) 👉 *(Internal link: **Viral Pneumonia – Causes, Symptoms & Treatment**)* ### Mode of Spread * Respiratory droplets (coughing, sneezing, talking) * Close personal contact * Contaminated surfaces ### Contagious Period * **1–2 days before symptoms** * **5–7 days after symptom onset** * Longer in children and immunocompromised patients ### Key Point > Viral pneumonia spreads easily, especially in **crowded places, households, and hospitals**. --- ## 2️⃣ Bacterial Pneumonia (Moderately Contagious) ### Common Causes * *Streptococcus pneumoniae* * *Haemophilus influenzae* * *Mycoplasma pneumoniae* * *Chlamydia pneumoniae* 👉 *(Internal link: **Bacterial Pneumonia – Diagnosis & Antibiotic Management**)* ### Spread * Respiratory droplets * Close contact with infected person ⚠️ **Important:** You may catch the bacteria, but **only susceptible individuals develop pneumonia**. ### After Treatment * **Not contagious after 24–48 hours of effective antibiotics** --- ## 3️⃣ Aspiration Pneumonia (Not Contagious) ### Cause * Inhalation of: * Food particles * Vomit * Gastric acid * Oropharyngeal secretions 👉 *(Internal link: **Aspiration Pneumonia – Risk Factors & Prevention**)* ### Common in * Stroke patients * Alcohol intoxication * Elderly with swallowing disorders * ICU patients ❌ **No person-to-person spread** --- ## 4️⃣ Fungal Pneumonia (Not Contagious) ### Causes * *Histoplasma* * *Coccidioides* * *Aspergillus* 👉 *(Internal link: **Fungal Lung Infections – Clinical Features & Treatment**)* ### Transmission * Inhalation of spores from: * Soil * Bird or bat droppings * ❌ **No human-to-human transmission** --- ## 👥 Who Is More Likely to Get Pneumonia After Exposure? * Infants & elderly * Smokers * COPD or asthma patients * Diabetes mellitus * Immunocompromised (HIV, chemotherapy, steroids) 👉 *(Internal link: **Risk Factors for Severe Pneumonia**)* --- ## 🛡️ How to Prevent Spread of Contagious Pneumonia * Hand hygiene 🧼 * Mask use during respiratory illness 😷 * Cover mouth while coughing/sneezing * Avoid close contact during active infection * Vaccination: * **Influenza vaccine** * **Pneumococcal vaccine** * **COVID-19 vaccine** 👉 *(Internal link: **Vaccines That Prevent Pneumonia**)* --- ## 🧠 Key Takeaway > **Pneumonia is contagious only when caused by infectious agents like viruses or bacteria.** > Aspiration and fungal pneumonias **do not spread from person to person**. --- ## 🔗 Suggested Internal Linking Structure (SEO Boost) Use internal links to: * Pneumonia Types * Viral vs Bacterial Pneumonia * Pneumonia Symptoms * Pneumonia Diagnosis * Pneumonia Treatment Guidelines * Pneumonia Complications * Pneumonia Prevention & Vaccination This improves **topical authority**, **crawl depth**, and **search ranking**. --- If you want, I can next: * Add **HTML internal link anchors** for your site * Create **schema-ready medical content** * Generate **SEO title, meta description & keywords** * Convert this into **exam-oriented notes or patient-friendly version** Just tell me what you want next 👍

Rh-Negative Pregnancy: Causes, Risks, Anti-D Prophylaxis, Diagnosis & Complete Management Guide
Below is a **complete, concise-but-exhaustive medical reference** for **Rh-negative pregnancy**, followed by **SEO title, description, keywords**, and an **auto-generated image**. --- # ⭐ **RH-NEGATIVE PREGNANCY — COMPLETE DETAILS**   --- If you want, I can also create: ✅ **25 Hard Case-based MCQs (HTML/CSS/JS exam mode)** ✅ Flowcharts for diagnosis & management ✅ A printable PDF for your Medical Hub app Just tell me!

Liver Disorders in Pregnancy: Causes, Symptoms, Diagnosis & Management | Complete Guide
# **Liver Disorders in Pregnancy — Complete, Exam-Ready Medical Reference** Below is a **single-place, concise but exhaustive** medical summary covering **definition, pathophysiology, causes, clinical features, investigations, differential diagnoses, and full management** of all major liver disorders specific to pregnancy. --- # **1. Classification of Liver Disorders in Pregnancy** ## **A. Disorders Unique to Pregnancy** 1. **Hyperemesis Gravidarum (HG) with hepatic dysfunction** 2. **Intrahepatic Cholestasis of Pregnancy (ICP)** 3. **Pre-eclampsia related liver dysfunction** 4. **HELLP Syndrome** 5. **Acute Fatty Liver of Pregnancy (AFLP)** ## **B. Pre-existing Liver Diseases Aggravated by Pregnancy** * Viral hepatitis (A, B, C, E) * Autoimmune hepatitis * Wilson disease * Cirrhosis/portal hypertension ## **C. Coincidental Liver Disorders** * Gallstones, biliary colic * Acute cholecystitis * Drug-induced hepatotoxicity --- # **2. Hyperemesis Gravidarum (HG)** ### **Definition** Severe nausea/vomiting in early pregnancy → dehydration, ketosis, >5% weight loss, with mild ↑LFTs. ### **Pathophysiology** * High **β-hCG and estrogen** → trigger vomiting center * Starvation → hepatic stress → mild ↑AST/ALT ### **Clinical Features** * Persistent vomiting * Dehydration, tachycardia * Mild jaundice (rare) ### **Investigations** * LFTs: ALT/AST mildly ↑ (usually <300 IU/L) * Electrolytes: ↓K⁺, ↓Na⁺ * Ketonuria ### **Differentials** * ICP * Hepatitis * GI obstruction ### **Management** * IV fluids (NS + thiamine BEFORE dextrose) * Antiemetics: * **Ondansetron** (5-HT₃ antagonist) * **Doxylamine + pyridoxine** * **Metoclopramide** * Manage electrolytes * Rarely hospitalisation + enteral/parenteral feeding --- # **3. Intrahepatic Cholestasis of Pregnancy (ICP)** ### **Definition** Reversible **hormone-triggered cholestasis** in 2nd–3rd trimester → **generalized pruritus**, ↑serum bile acids. ### **Pathophysiology** * Estrogen → ↓bile flow * Genetic factors (ABCB4, ABCB11 mutations) * Accumulation of **bile acids → placental vasoconstriction** ### **Clinical Features** * Severe **itching**, especially palms/soles * No rash * Mild jaundice (10–20%) ### **Investigations** * **Serum bile acids >10–14 µmol/L** = diagnostic * ALT/AST mildly ↑ * Bilirubin normal/slightly ↑ ### **Differentials** * Viral hepatitis * Drug-induced cholestasis * AFLP / HELLP ### **Management** **Maternal** * **Ursodeoxycholic acid (UDCA)**: 10–15 mg/kg/day * Improves bile flow, reduces pruritus * Antihistamines for itch * Vitamin K supplementation if prolonged PT **Fetal** * Weekly NST/BPP * **Delivery at 36–37 weeks** to prevent stillbirth --- # **4. Pre-eclampsia-Related Liver Dysfunction** ### **Mechanism** Generalized endothelial dysfunction → hepatic vasospasm → ischemia → periportal necrosis → ↑LFTs. ### **Features** * Hypertension, proteinuria * RUQ/epigastric pain * Mild ↑AST/ALT (<300 IU/L) ### **Management** * Control BP (labetalol, hydralazine) * Magnesium sulfate for seizure prophylaxis * **Delivery = definitive treatment** --- # **5. HELLP Syndrome** (Hemolysis, Elevated Liver enzymes, Low Platelets) ### **Pathophysiology** Microangiopathic hemolysis + hepatic sinusoidal obstruction → liver ischemia → ↑LFTs + thrombocytopenia. ### **Clinical Features** * RUQ pain * Nausea/vomiting * Hypertension ± proteinuria * Jaundice (mild) ### **Investigations** * AST/ALT ↑ (usually 300–1000 IU/L) * Platelets <100,000 * ↑LDH, ↑bilirubin * Schistocytes on smear ### **Management** * Stabilize mother * Magnesium sulfate * Control BP * **Immediate delivery** (≥34 weeks or earlier if unstable) * Platelet transfusion if <20,000 or surgery needed --- # **6. Acute Fatty Liver of Pregnancy (AFLP)** **Most severe pregnancy-specific liver disorder** ### **Definition** Acute microvesicular fatty infiltration of hepatocytes → **acute liver failure** in 3rd trimester. ### **Pathophysiology** * Mitochondrial **fatty acid oxidation defect** (LCHAD deficiency in fetus) * Maternal inability to metabolize fatty acids → toxic metabolites → hepatic failure ### **Clinical Features** * Prodrome: nausea, vomiting * **Jaundice prominent** * **Hypoglycemia** * **Encephalopathy** * Polyuria/polydipsia (diabetes insipidus-like) * Coagulopathy, DIC ### **Investigations** * AST/ALT moderately ↑ (300–500 IU/L) * **Hypoglycemia** * ↑Ammonia * ↑Bilirubin * **Prolonged PT/INR** * Leukocytosis * US: bright fatty liver (not always) ### **Differentials** * HELLP * Severe hepatitis * Sepsis ### **Management** * **Immediate delivery — life-saving** * ICU care * Manage hypoglycemia (IV dextrose) * Correct coagulopathy (FFP, cryoprecipitate) * Treat encephalopathy (lactulose) --- # **7. Viral Hepatitis in Pregnancy** ### **Key Points** * **Hepatitis E** → highest maternal mortality (up to 20–30%) * Hepatitis B transmission risk highest if HBeAg positive ### **Features** * Markedly raised LFTs * Jaundice * Coagulopathy (severe cases) ### **Management** * Supportive * **Hepatitis B**: give **HBIG + vaccine** to newborn * Avoid ribavirin in pregnancy --- # **8. Gallstone Disease and Acute Cholecystitis** ### **Pathophysiology** Progesterone → biliary stasis Estrogen → ↑cholesterol in bile → gallstones ### **Features** * RUQ pain * Fever (in cholecystitis) * Nausea/vomiting ### **Investigations** * US abdomen: first-line ### **Management** * Pain control * IV antibiotics (cephalosporins safe) * ERCP if choledocholithiasis * Cholecystectomy (2nd trimester safest) --- # **9. Differentiating HELLP vs AFLP vs ICP** | Feature | HELLP | AFLP | ICP | | ---------------- | --------- | --------- | ------------- | | Jaundice | Mild | Prominent | Mild | | Platelets | ↓↓↓ | Mild ↓ | Normal | | Glucose | Normal | **Low** | Normal | | Bile acids | Normal | Normal | **Very high** | | Delivery urgency | Immediate | Immediate | 36–37 weeks | --- # **10. Summary of Management Principles** ### **A. Maternal stabilization** * Correct fluids, electrolytes * Manage coagulation issues * BP control * Seizure prophylaxis where indicated ### **B. Fetal monitoring** * NST, BPP, Doppler * Early delivery if maternal/fetal compromise ### **C. Delivery** * ICP → 36–37 weeks * HELLP/AFLP → **immediate** --- If you want, I can also generate: ✅ **SEO title + description + keywords** ✅ **Stylish HTML/CSS/JS MCQs (hard, case-based)** ✅ **Flowcharts / diagrams** ✅ **An image illustration** Just tell me **what you want next**.

Pregnancy-Induced Hypertension (PIH): Complete Causes, Symptoms, Diagnosis & Treatment Guide
Below is a **complete, concise-but-exhaustive, exam-ready medical reference** on **Pregnancy-Induced Hypertension (PIH)**—also called **gestational hypertension**. Covers: **definition, pathophysiology, etiologies, risk factors, clinical features, investigations, differential diagnosis, complications (maternal & fetal), management (stepwise), drugs with dosing + MOA + AEs + contraindications + monitoring**, delivery timing, prevention, counseling. --- # ⭐ **PREGNANCY-INDUCED HYPERTENSION (PIH) — COMPLETE DETAILS** ! --- # **1️⃣ Definition** **PIH = Gestational Hypertension** * **BP ≥140/90 mmHg** after **20 weeks** of pregnancy * **No proteinuria** * **No features of end-organ dysfunction** * BP becomes normal within **12 weeks postpartum** --- # **2️⃣ Epidemiology** * Occurs in **6–10%** of pregnancies * More common in **primigravida**, **multiple gestation**, **teenage pregnancy**, **advanced maternal age** --- # **3️⃣ Etiology & Risk Factors** ### **Major Risk Factors** * Primigravida * Family history of PIH/Preeclampsia * Personal history of PIH * Multiple pregnancy * Molar pregnancy * Diabetes, Obesity, Chronic hypertension * Autoimmune disease * Renal disease * Thrombophilias * Advanced maternal age (>35 years) --- # **4️⃣ Pathophysiology (Simplified & Complete)**   ### **Normal Pregnancy** * Trophoblast invades → spiral arteries remodel → become wide, low-resistance → good placental perfusion. ### **PIH / Preeclampsia Spectrum** 1. **Defective trophoblastic invasion** → incomplete spiral artery remodeling 2. **Placental ischemia** → oxidative stress 3. **Release of antiangiogenic factors** (sFlt-1, endoglin) and inflammatory mediators 4. **Maternal endothelial dysfunction** → * ↑ vascular resistance * ↑ capillary permeability * Hypercoagulability 🔹 **PIH = mild endotheliopathy without proteinuria or organ dysfunction** 🔹 **Preeclampsia = PIH + proteinuria or organ dysfunction** --- # **5️⃣ Diagnostic Criteria** ### **BP Measurement** * Two readings ≥140/90 mmHg * At least 4 hours apart * After 20 weeks gestation * No proteinuria * No systemic symptoms ### **Proteinuria must be absent** * Dipstick <1+ * Spot urine protein/creatinine ratio <0.3 * 24-hr urinary protein <300 mg --- # **6️⃣ Clinical Features** ### **Usually Asymptomatic** Detected on routine antenatal screening. ### **If symptoms appear** * Headache * Mild pedal edema * Dizziness * Visual disturbances (suggest severe disease progression) * Epigastric pain (danger sign) --- # **7️⃣ Investigations (Complete Panel)** ### **Basic** * BP monitoring * Urinalysis (protein) * CBC * LFTs (AST/ALT) * Renal function test (creatinine, uric acid) ### **For progression to Preeclampsia** * Urine PCR * Peripheral smear (hemolysis) * Coagulation profile * LDH * Fundus examination ### **Fetal Evaluation** * Ultrasound for growth * AFI * Doppler velocimetry * NST / BPP --- # **8️⃣ Differential Diagnosis** * **Chronic hypertension** * **White coat hypertension** * **Preeclampsia** * **Transient hypertension of pregnancy** * **Renal disease** * **Thyroid disorders** * **Drug-induced hypertension** --- # **9️⃣ Maternal Complications** ### **If PIH progresses → Preeclampsia/Eclampsia** * Severe hypertension * HELLP syndrome * DIC * Acute renal failure * Pulmonary edema * Placental abruption * Eclampsia * Stroke / Intracranial hemorrhage --- # **🔟 Fetal Complications** * IUGR * Oligohydramnios * Preterm birth * Fetal hypoxia * Placental insufficiency * Stillbirth --- # **1️⃣1️⃣ Management (Complete Stepwise Protocol)**   --- ## **A. General Measures** * Rest, preferably left lateral * Reduce physical stress * Salt restriction **NOT** recommended severely, only normal diet * Daily fetal movement count * Regular BP monitoring * Weekly ANC visits --- ## **B. Threshold for Treatment** * **Treat if BP ≥150/100 mmHg** * For **140–149/90–99 → Monitor only**, no medication unless comorbidity --- ## **C. First-Line Antihypertensive Drugs in Pregnancy** --- # **🔹1. Labetalol (Drug of Choice)** **MOA:** α-1 & β-blocker → ↓ SVR & BP **Dose:** * Oral: 100–200 mg twice daily → up to 2,400 mg/day * IV (for severe): 20 mg bolus → 40 mg → 80 mg q10min (max 300 mg) **PK:** Hepatic metabolism **Common AEs:** Fatigue, dizziness **Serious AEs:** Bradycardia, hypotension **Contraindications:** Asthma, heart block **Monitoring:** BP, HR **Counselling:** Avoid abrupt stopping --- # **🔹2. Nifedipine (Long-acting)** **MOA:** Calcium channel blocker → vasodilation **Dose:** 30–60 mg sustained-release OD **PK:** Hepatic **Common AEs:** Headache, flushing **Serious AEs:** Hypotension **Contraindications:** Aortic stenosis **Interactions:** Magnesium sulfate ↑ hypotension risk **Monitoring:** BP **Counselling:** Do not chew CR tablets --- # **🔹3. Methyldopa (Safe in pregnancy)** **MOA:** Central α2 agonist **Dose:** 250–500 mg 2–3 times/day **PK:** Renal **Common AEs:** Sedation, depression, dry mouth **Serious AEs:** Liver dysfunction, hemolytic anemia **Monitoring:** LFTs **Counselling:** May cause drowsiness --- # ❌ **Drugs Contraindicated** * ACE inhibitors * ARBs * Atenolol * Diuretics (except pulmonary edema) --- # **1️⃣2️⃣ Management of Severe PIH** * BP ≥160/110 mmHg * Admit * IV labetalol / oral nifedipine * Evaluate for preeclampsia * Magnesium sulfate if criteria for severe features --- # **1️⃣3️⃣ Magnesium Sulfate (for progression to severe/eclampsia)** **MOA:** CNS depressant → prevents seizures by NMDA blockade **Dose (Pritchard):** * 4 g IV loading + 10 g IM (5 g each buttock) * 5 g IM q4h **Monitoring:** * Respiratory rate * Urine output (>30 ml/hr) * Patellar reflex **Toxicity:** Respiratory depression → treat with **10% calcium gluconate 10 ml IV** --- # **1️⃣4️⃣ Delivery Timing** | Condition | Timing | | ------------------------------------------------ | ------------------------- | | **PIH (controlled)** | **37 weeks** | | **Severe PIH** | 34 weeks (after steroids) | | **Uncontrolled BP, fetal compromise, abruption** | Immediate delivery | --- # **1️⃣5️⃣ Intrapartum Care** * Continuous fetal monitoring * Keep BP <160/110 * Avoid fluid overload * Anesthesia: regional preferred unless contraindicated --- # **1️⃣6️⃣ Postpartum Care** * Continue antihypertensives * Monitor BP for **12 weeks** * If persistent → chronic hypertension --- # **1️⃣7️⃣ Prevention of PIH** * Low-dose **Aspirin 75–150 mg at bedtime** from **12–16 weeks** in high-risk women * Calcium supplementation (1–1.5 g/day) in low-calcium diets * Weight control * Control comorbidities --- # **1️⃣8️⃣ Patient Counseling Points** * Regular BP monitoring * Danger signs: headache, visual symptoms, epigastric pain * Adherence to medications * Fetal kick count * Importance of follow-up * No self-discontinuation of drugs --- # ⭐ If you want, I can also provide: ✅ **Flowchart of PIH diagnosis** ✅ **Flowchart of management** ✅ **HTML/CSS/JS quiz (hard, case-based)** ✅ **SEO title + description + keywords** ✅ **Image generation** Just tell me what you need next!
Browse by Medical Category
Explore content organized by medical specialties and systems