Carpal Tunnel Syndrome: Symptoms, Nerve Conduction Study & Treatment Algorithm
Orthopedics
0 ❤
0 💬
By dinesh_01
# **Carpal Tunnel Syndrome (CTS): Symptoms, Nerve Conduction Study & Treatment Algorithm**
## **Definition**
Carpal Tunnel Syndrome is **median nerve compression** at the level of the wrist within the **carpal tunnel**, leading to sensory and motor dysfunction in the **median nerve distribution**.
---
# **Pathophysiology**
* The **carpal tunnel** is a rigid space bordered by carpal bones and the **transverse carpal ligament**.
* Conditions causing tunnel **volume increase** or **nerve vulnerability** → median nerve ischemia + demyelination.
* Chronic compression → **axonal loss** → persistent weakness and atrophy.
---
# **Causes / Risk Factors**
### **Local / Mechanical**
* Repetitive wrist flexion/extension
* Vibrating tool use
* Wrist fractures/dislocations
* Ganglion cysts, synovitis
### **Systemic**
* Diabetes mellitus
* Hypothyroidism
* Pregnancy (fluid retention)
* Rheumatoid arthritis
* Obesity
* Amyloidosis
---
# **Clinical Features**
### **Symptoms**
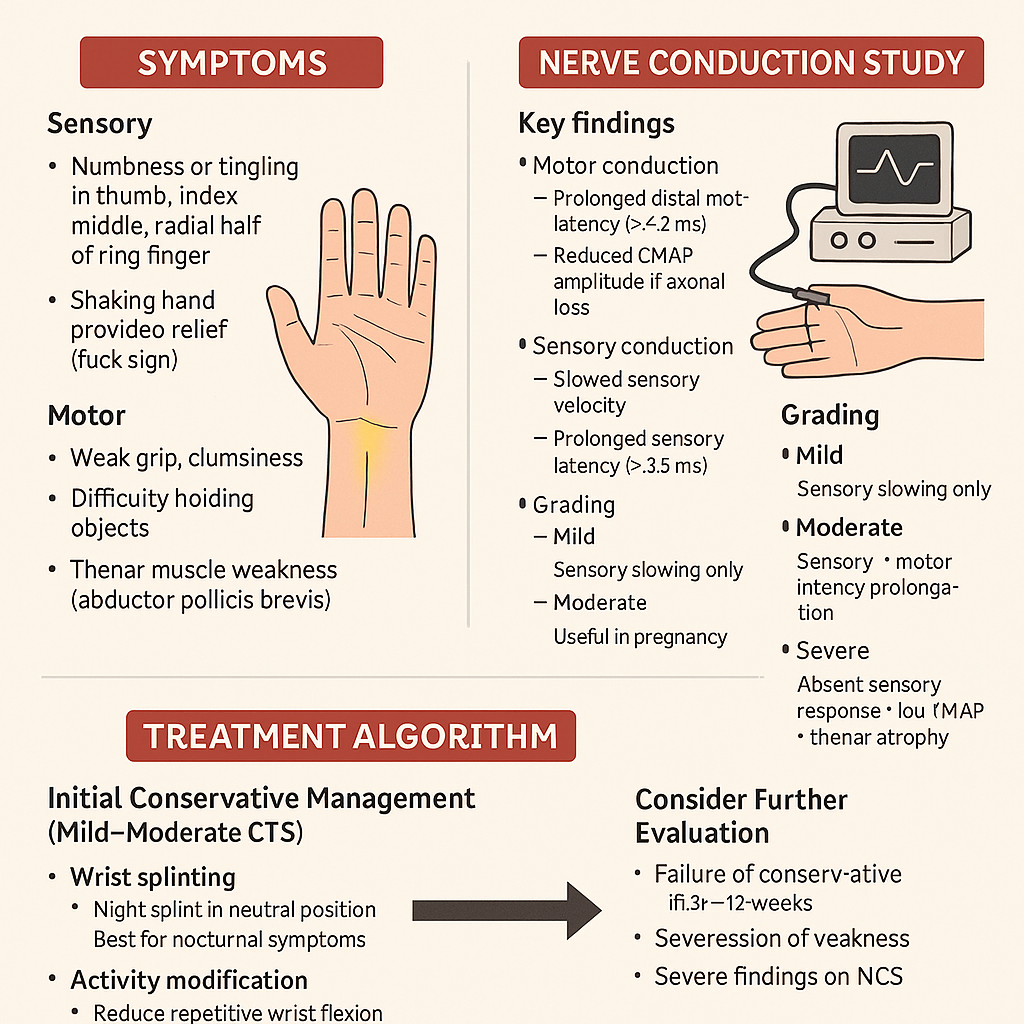
**Sensory:**
* Numbness/tingling in **thumb, index, middle, radial half of ring finger**
* Symptoms worse at **night**
* **Shaking hand provides relief** (flick sign)
**Motor:**
* Weak grip, clumsiness
* Difficulty holding objects
* **Thenar muscle weakness** (abductor pollicis brevis)
**Autonomic signs (less common):**
* Dryness of skin over lateral 3½ fingers
---
### **Physical Examination**
* **Tinel’s sign:** Tapping over carpal tunnel → tingling in median nerve area
* **Phalen’s test:** Forced wrist flexion for 60 sec → reproduces symptoms
* **Durkan’s test (carpal compression test):** Direct pressure over the tunnel → most sensitive
* Thenar muscle **atrophy** in advanced disease
---
# **Nerve Conduction Study (NCS) — Key Findings**
NCS is the **gold standard**.
### **Motor conduction**
* Prolonged **distal motor latency** (> 4.2 ms) of median nerve
* Reduced CMAP amplitude if axonal loss
### **Sensory conduction**
* Slowed sensory velocity
* Prolonged **sensory latency** (> 3.5 ms)
* Reduced SNAP amplitude
### **Comparison tests**
* Median vs ulnar sensory latency to ring finger
* Median–radial latency difference to thumb
* Very sensitive in early disease
### **Grading**
* **Mild:** Sensory slowing only
* **Moderate:** Sensory + motor latency prolongation
* **Severe:** Absent sensory response + low CMAP + thenar atrophy
---
# **Diagnosis**
* Clinical examination + NCS
* Ultrasound: Median nerve cross-sectional area > **9–10 mm²** at carpal tunnel inlet
* X-ray only if trauma suspected
* Rule out differentials: cervical radiculopathy (C6), pronator syndrome, diabetic polyneuropathy
---
# **Treatment Algorithm (Stepwise)**
## **1. Initial Conservative Management (Mild–Moderate CTS)**
### **a. Wrist Splinting**
* **Night splint** in neutral position
* Best first-line for nocturnal symptoms
### **b. Activity Modification**
* Reduce repetitive wrist flexion
* Ergonomic adjustments
### **c. NSAIDs**
* Provides symptom relief, but **does not alter nerve pathology**
### **d. Corticosteroid Injection**
* Local steroid injection gives **weeks–months of relief**
* Useful in pregnancy
* Avoid frequent injections (>3/year)
---
## **2. Consider Further Evaluation**
* Failure of conservative therapy in **6–12 weeks**
* Progression of weakness
* Severe findings on NCS
---
## **3. Definitive Treatment — Surgery**
### **Surgical Indication**
* Persistent symptoms despite conservative therapy
* Severe CTS (thenar atrophy or axonal loss on NCS)
* Recurrent symptoms significantly affecting function
### **Procedure**
**Carpal Tunnel Release (CTR)**
* Cut the transverse carpal ligament to decompress the median nerve
* Approaches: **open** or **endoscopic**
### **Outcomes**
* Excellent symptom improvement in majority
* Thenar strength recovery depends on duration of compression
* Recurrence is uncommon
---
# **Prognosis**
* Early-stage CTS responds well to conservative therapy
* Long-standing compression with axonal damage → incomplete recovery
* Diabetes: slower improvement
* Pregnancy: symptoms often resolve postpartum
---
# **Red Flags (Suggest Alternative Diagnosis)**
* Whole-hand numbness (not median distribution)
* Neck pain + hand paresthesia → cervical radiculopathy
* Symptoms not affected by wrist position
* Marked weakness without sensory loss → motor neuron or peripheral nerve disorder
---
Comments & Discussion
Use this thread like a mini viva: add differentials, staging systems, drug regimens and exam tricks.
Login or register to comment.
No comments yet – start by adding exam-style discussion points.